Leptospirosis laboratory findings: Difference between revisions
m (Bot: Removing from Primary care) |
|||
| (56 intermediate revisions by 6 users not shown) | |||
| Line 1: | Line 1: | ||
__NOTOC__ | __NOTOC__ | ||
[[Image:Leptospirosis in kidney.jpg|thumb|right|Kidney tissue, using a [[silver stain]]ing technique, revealing the presence of ''Leptospira'' bacteria - Public Domain, https://commons.wikimedia.org/w/index.php?curid=2256011]] | |||
{{Leptospirosis}} | {{Leptospirosis}} | ||
{{CMG}} | {{CMG}};{{AE}}{{VSKP}} | ||
==Overview== | ==Overview== | ||
The diagnosis of leptospirosis should be considered in a patient with a history of contact with potentially infected animals, soil or surface waters contaminated by animal urine. | The diagnosis of leptospirosis is based upon clinical suspicion and lab findings, so lab tests should be considered in a patient with a history of contact with potentially [[infected]] animals, [[soil]] or surface waters contaminated by animal [[urine]].<ref name="pmid22843698">{{cite journal| author=Forbes AE, Zochowski WJ, Dubrey SW, Sivaprakasam V| title=Leptospirosis and Weil's disease in the UK. | journal=QJM | year= 2012 | volume= 105 | issue= 12 | pages= 1151-62 | pmid=22843698 | doi=10.1093/qjmed/hcs145 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=22843698 }} </ref> Leptospires can be found in [[blood]] and [[CSF]] for the first 7 to 10 days and then in the [[urine]]. Hence, in the early diagnosis, specimen of choice should be [[blood]] or [[CSF]] for [[culture]]. From the second week onwards serological tests are useful in the diagnosis. | ||
==Laboratory findings== | ==Laboratory findings== | ||
===Laboratory Findings=== | |||
As the clinical manifestations of the disease are non specific, the clinical diagnosis is difficult. The laboratory investigations for leptospirosis should be considered in patient with an abrupt onset of [[fever]], [[chills]], [[conjunctival]] suffusion, [[headache]], [[myalgia]] and [[jaundice]] with history of occupational exposure to [[infected]] animals or contaminated with animal urine.<ref>{{cite book | last = LastName | first = FirstName | title = Human leptospirosis : guidance for diagnosis, surveillance and control | publisher = World Health Organization | location = Geneva | year = 2003 | isbn = 9241545895 }}</ref> | |||
[[ | |||
Laboratory investigations useful in the diagnosis of leptospirosis include: | |||
* Identification of leptospires in tissues using [[antibodies]] labelled with fluorescent markers | |||
* [[Antibody]] detection by serological studies | |||
* Culture the [[bacteria]] from [[blood]], [[urine]] or [[tissues]] | |||
* Other methods such as [[PCR]][[Immunostaining|Iandmmunostaining]]. | |||
Laboratory criteria for the diagnosis of leptospirosis are presence of one or more of the following:<ref name="pmid22843698">{{cite journal| author=Forbes AE, Zochowski WJ, Dubrey SW, Sivaprakasam V| title=Leptospirosis and Weil's disease in the UK. | journal=QJM | year= 2012 | volume= 105 | issue= 12 | pages= 1151-62 | pmid=22843698 | doi=10.1093/qjmed/hcs145 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=22843698 }} </ref> | |||
'''Presumptive diagnosis:''' | |||
* A positive result in [[IgM]] serological tests, slide [[agglutination]] test or [[latex agglutination test]] or immunochromatographic test. | |||
* A microscopic [[agglutination]] test (MAT) titre of 100/200/400 or above in single sample based on test. | |||
* Identification of leptospires directly or by staining methods. | |||
'''Confirmatory diagnosis:''' | |||
* Culture positivity | * Culture positivity | ||
* Antibody titre of ≥1 in 320 by Microscopic Agglutination test (MAT) in a single serum sample | * [[Antibody]] titre of ≥1 in 320 by Microscopic Agglutination test (MAT) in a single serum sample | ||
* Seroconversion in paired sera collected in the acute and convalescent phase established by ELISA IgM and/or MAT methods | * Seroconversion in paired sera collected in the acute and convalescent phase established by [[ELISA]] [[IgM]] and/or MAT methods | ||
* Evidence of leptospira antigen by molecular methods. | * Evidence of [[leptospira]] [[antigen]] by molecular methods.{{familytree/start}} | ||
Laboratory investigations | {{familytree | | | | | | | | C02 | | | | | | | |C02=Laboratory investigations for leptospirosis}} | ||
* Identification of leptospires in | {{familytree | |,|-|-|-|v|-|-|^|-|-|v|-|-|-|.| | | }} | ||
* | {{familytree | D01 | | D02 | | | | D03 | | D04 |D01=Culture|D02=Microscopic|D03=Immunological|D04=Molecular}} | ||
* | {{familytree | |!| | | |!| | | | | |!| | | |!| | | }} | ||
* | {{familytree |boxstyle=text-align: left; | E01 | | E02 | | | | E04 | | E05 |E01=• Isolation|E02=• [[Dark field microscopy]]<br>• Immunofluoroscence microscopy|E04=• Microscopic [[agglutination]] test<br>• ELISA test<br>• [[Latex agglutination test]]|E05=• [[Polymerase chain reaction]]}} | ||
{{familytree/end}} | |||
===Blood Tests=== | |||
Blood tests in leptospirosis include:<ref name="pmid13819407">{{cite journal| author=EDWARDS GA, DOMM BM| title=Human leptospirosis. | journal=Medicine (Baltimore) | year= 1960 | volume= 39 | issue= | pages= 117-56 | pmid=13819407 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=13819407 }} </ref> | |||
* '''CBC:''' Peripheral [[leukocytosis]] with a left shift, [[thrombocytopenia]], | |||
* Elevated [[Erythrocyte sedimentation rate|ESR]] | |||
* '''Liver functional tests:''' Mild elevation in [[aminotransferases]], [[bilirubin]], and [[alkaline phosphatase]].<ref name="pmid14652202">{{cite journal| author=Bharti AR, Nally JE, Ricaldi JN, Matthias MA, Diaz MM, Lovett MA et al.| title=Leptospirosis: a zoonotic disease of global importance. | journal=Lancet Infect Dis | year= 2003 | volume= 3 | issue= 12 | pages= 757-71 | pmid=14652202 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=14652202 }} </ref> | |||
* Elevated plasma [[creatinine]], elevated [[blood urea nitrogen]](BUN) | |||
* Elevated [[creatinine phosphokinase]] (CPK) | |||
===Urinalysis=== | |||
* [[Proteinuria]] | |||
* [[Pyuria]] | |||
* [[Microscopic hematuria]] | |||
* [[Hyaline]] and granular [[Casts in urine|casts]] | |||
===CSF Analysis === | |||
[[CSF]] findings are common in first or second week of illness.<ref name="pmid14902167">{{cite journal| author=BEESON PB, HANKEY DD| title=Leptospiral meningitis. | journal=AMA Arch Intern Med | year= 1952 | volume= 89 | issue= 4 | pages= 575-83 | pmid=14902167 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=14902167 }} </ref> | |||
* Opening pressure: normal or slightly elevated | |||
* Cells: [[Lymphocyte]] predominance<ref name="pmid14902167">{{cite journal| author=BEESON PB, HANKEY DD| title=Leptospiral meningitis. | journal=AMA Arch Intern Med | year= 1952 | volume= 89 | issue= 4 | pages= 575-83 | pmid=14902167 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=14902167 }} </ref> | |||
* [[Protein]]: Normal to elevated<ref name="pmid13819407">{{cite journal| author=EDWARDS GA, DOMM BM| title=Human leptospirosis. | journal=Medicine (Baltimore) | year= 1960 | volume= 39 | issue= | pages= 117-56 | pmid=13819407 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=13819407 }} </ref> | |||
* [[Glucose]]: Normal | |||
* Xanthochromasia is seen in severe Icteric leptospirosis<ref name="pmid20263193">{{cite journal| author=CARGILL WH, BEESON PB| title=The value of spinal fluid examination as a diagnostic procedure in Weil's disease. | journal=Ann Intern Med | year= 1947 | volume= 27 | issue= 3 | pages= 396-400 | pmid=20263193 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=20263193 }} </ref> | |||
=== Isolation of Leptospires === | |||
Isolation of leptospires from clinical specimens is the strongest evidence for confirmation of leptospirosis. Leptospira can be cultured in Ellinghausen-McCullough-Johnson-Harris medium, which is incubated at 28 to 30ºC.<ref name="pmid3754265">{{cite journal| author=Rule PL, Alexander AD| title=Gellan gum as a substitute for agar in leptospiral media. | journal=J Clin Microbiol | year= 1986 | volume= 23 | issue= 3 | pages= 500-4 | pmid=3754265 | doi= | pmc=268682 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=3754265 }} </ref> The median time to positivity is three weeks with a maximum of 3 months. This makes culture techniques useless for diagnostic purposes, but is commonly used in research. | |||
'''Blood culture:''' | |||
* Should be done before starting of [[antibiotics]] | |||
* Useful if done with in 10days after the initial presentation.<ref name="pmid7989538">{{cite journal| author=Bal AE, Gravekamp C, Hartskeerl RA, De Meza-Brewster J, Korver H, Terpstra WJ| title=Detection of leptospires in urine by PCR for early diagnosis of leptospirosis. | journal=J Clin Microbiol | year= 1994 | volume= 32 | issue= 8 | pages= 1894-8 | pmid=7989538 | doi= | pmc=263898 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=7989538 }} </ref> | |||
'''Urine culture:''' | |||
* Should be tested between 10-30days of initial presentaion | |||
* Sample should be tested within 2hours of collection | |||
'''CSF culture:''' | |||
* Should be tested between 5-10days of initial presentaion | |||
===Identification of Leptospires=== | |||
'''Dark field microscopy:''' In order to detect under [[dark field microscopy]] 10<sup>4</sup> leptospires/ml are necessary for one cell per field. | |||
* Specimen: [[Blood]], [[urine]], [[CSF]] | |||
* Disadvantages: Test is insensitive and lacks specificity | |||
[[File:Leptospirosis Darkfield Microscopy.jpg|300px|thumb|center|Leptospira Dark field microscopy finding - By bluuurgh - Own work, Public Domain, https://commons.wikimedia.org/w/index.php?curid=1534679]] | |||
'''Other microscopic techniques:''' Immunofluoroscence, [[Light microscopy]] | |||
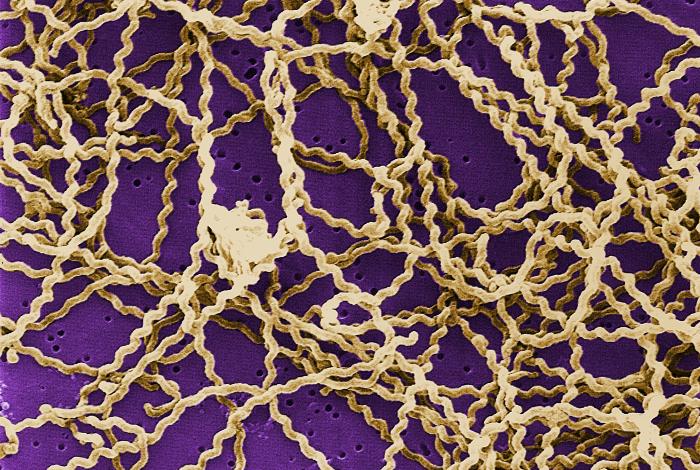
[[File:Leptospira Electron Microscopy.jpg|thumb|center|300px|Leptospira Electron microscopy finding - By CDC/ Rob Weyant - http://phil.cdc.gov/PHIL_Images/20050308/22ad4ce53a1648feb011a7d6dd26fbb6/138_lores.jpg, Public Domain, https://commons.wikimedia.org/w/index.php?curid=611941]] | |||
=== Detection of specic antibodies of leptospires or Serological tests === | |||
Serological test are useful to detect leptospira-specific [[Immunoglobulin M|IgM]] [[antibodies]] in the early acute phase of [[illness]], especially after first week of clinical symptoms. Antibodies production start 5-7 days after the onset of the initial presentation. [[Serological testing|Serological test]] in the 1st week will give false negative results. | |||
<br>'''Screening tests''' | |||
* [[Enzyme linked immunosorbent assay (ELISA)|Enzyme-linked immunosorbent assay]] (ELISA): [[Sensitivity (test)|sensitivity]] of 90% and [[Specificity (tests)|specificity]] of 94%.<ref name="pmid11271784">{{cite journal| author=Zochowski WJ, Palmer MF, Coleman TJ| title=An evaluation of three commercial kits for use as screening methods for the detection of leptospiral antibodies in the UK. | journal=J Clin Pathol | year= 2001 | volume= 54 | issue= 1 | pages= 25-30 | pmid=11271784 | doi= | pmc=1731274 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=11271784 }} </ref> Positive test results shows high [[Immunoglobulin M|IgM]] titre in a single serum sample or a 4-fold rise in titre in a paired tests is consistent with current or recent infection. | |||
** Advantages: Single [[antigenic]] preparation can be used. Allows rapid processing of large number of samples. | |||
* Rapid diagnostic tests: Latex based agglutination test, Immunochromatography. | |||
'''Confirmatory tests''' | |||
* Microscopic agglutination test (MAT): [[Specificity]] of 94%. All positive screening tests should be confirmed by the MAT. Agglutinating [[antibodies]] can detects both [[IgM]] and [[IgG]] classes and are detectable from about days 7 to 10 after onset of symptoms. | |||
** Advantages : It is serovar specific test. Once infected the person stays MAT positive for several years so the test is useful for epidemiological purpose. | |||
=== Molecular Diagnosis === | |||
=== Polymerase Chain Reaction === | |||
[[Polymerase chain reaction]] will give quick results in the early stage of the disease when antibodies have not yet developed in detectable levels (<7 days) | |||
==References== | ==References== | ||
| Line 31: | Line 97: | ||
[[Category:Disease]] | [[Category:Disease]] | ||
[[Category:Emergency mdicine]] | |||
[[Category:Up-To-Date]] | |||
[[Category:Infectious disease]] | [[Category:Infectious disease]] | ||
[[Category:Pulmonology]] | |||
[[Category:Gastroenterology]] | |||
[[Category:Otolaryngology]] | |||
[[Category:Neurology]] | |||
Latest revision as of 22:29, 29 July 2020

|
Leptospirosis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Leptospirosis laboratory findings On the Web |
|
American Roentgen Ray Society Images of Leptospirosis laboratory findings |
|
Risk calculators and risk factors for Leptospirosis laboratory findings |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Venkata Sivakrishna Kumar Pulivarthi M.B.B.S [2]
Overview
The diagnosis of leptospirosis is based upon clinical suspicion and lab findings, so lab tests should be considered in a patient with a history of contact with potentially infected animals, soil or surface waters contaminated by animal urine.[1] Leptospires can be found in blood and CSF for the first 7 to 10 days and then in the urine. Hence, in the early diagnosis, specimen of choice should be blood or CSF for culture. From the second week onwards serological tests are useful in the diagnosis.
Laboratory findings
Laboratory Findings
As the clinical manifestations of the disease are non specific, the clinical diagnosis is difficult. The laboratory investigations for leptospirosis should be considered in patient with an abrupt onset of fever, chills, conjunctival suffusion, headache, myalgia and jaundice with history of occupational exposure to infected animals or contaminated with animal urine.[2]
Laboratory investigations useful in the diagnosis of leptospirosis include:
- Identification of leptospires in tissues using antibodies labelled with fluorescent markers
- Antibody detection by serological studies
- Culture the bacteria from blood, urine or tissues
- Other methods such as PCRIandmmunostaining.
Laboratory criteria for the diagnosis of leptospirosis are presence of one or more of the following:[1]
Presumptive diagnosis:
- A positive result in IgM serological tests, slide agglutination test or latex agglutination test or immunochromatographic test.
- A microscopic agglutination test (MAT) titre of 100/200/400 or above in single sample based on test.
- Identification of leptospires directly or by staining methods.
Confirmatory diagnosis:
- Culture positivity
- Antibody titre of ≥1 in 320 by Microscopic Agglutination test (MAT) in a single serum sample
- Seroconversion in paired sera collected in the acute and convalescent phase established by ELISA IgM and/or MAT methods
- Evidence of leptospira antigen by molecular methods.
Laboratory investigations for leptospirosis Culture Microscopic Immunological Molecular • Isolation • Dark field microscopy
• Immunofluoroscence microscopy• Microscopic agglutination test
• ELISA test
• Latex agglutination test• Polymerase chain reaction Blood Tests
Blood tests in leptospirosis include:[3]
- CBC: Peripheral leukocytosis with a left shift, thrombocytopenia,
- Elevated ESR
- Liver functional tests: Mild elevation in aminotransferases, bilirubin, and alkaline phosphatase.[4]
- Elevated plasma creatinine, elevated blood urea nitrogen(BUN)
- Elevated creatinine phosphokinase (CPK)
Urinalysis
- Proteinuria
- Pyuria
- Microscopic hematuria
- Hyaline and granular casts
CSF Analysis
CSF findings are common in first or second week of illness.[5]
- Opening pressure: normal or slightly elevated
- Cells: Lymphocyte predominance[5]
- Protein: Normal to elevated[3]
- Glucose: Normal
- Xanthochromasia is seen in severe Icteric leptospirosis[6]
Isolation of Leptospires
Isolation of leptospires from clinical specimens is the strongest evidence for confirmation of leptospirosis. Leptospira can be cultured in Ellinghausen-McCullough-Johnson-Harris medium, which is incubated at 28 to 30ºC.[7] The median time to positivity is three weeks with a maximum of 3 months. This makes culture techniques useless for diagnostic purposes, but is commonly used in research.
Blood culture:
- Should be done before starting of antibiotics
- Useful if done with in 10days after the initial presentation.[8]
Urine culture:
- Should be tested between 10-30days of initial presentaion
- Sample should be tested within 2hours of collection
CSF culture:
- Should be tested between 5-10days of initial presentaion
Identification of Leptospires
Dark field microscopy: In order to detect under dark field microscopy 104 leptospires/ml are necessary for one cell per field.

Leptospira Dark field microscopy finding - By bluuurgh - Own work, Public Domain, https://commons.wikimedia.org/w/index.php?curid=1534679 Other microscopic techniques: Immunofluoroscence, Light microscopy

Leptospira Electron microscopy finding - By CDC/ Rob Weyant - http://phil.cdc.gov/PHIL_Images/20050308/22ad4ce53a1648feb011a7d6dd26fbb6/138_lores.jpg, Public Domain, https://commons.wikimedia.org/w/index.php?curid=611941 Detection of specic antibodies of leptospires or Serological tests
Serological test are useful to detect leptospira-specific IgM antibodies in the early acute phase of illness, especially after first week of clinical symptoms. Antibodies production start 5-7 days after the onset of the initial presentation. Serological test in the 1st week will give false negative results.
Screening tests- Enzyme-linked immunosorbent assay (ELISA): sensitivity of 90% and specificity of 94%.[9] Positive test results shows high IgM titre in a single serum sample or a 4-fold rise in titre in a paired tests is consistent with current or recent infection.
- Advantages: Single antigenic preparation can be used. Allows rapid processing of large number of samples.
- Rapid diagnostic tests: Latex based agglutination test, Immunochromatography.
Confirmatory tests
- Microscopic agglutination test (MAT): Specificity of 94%. All positive screening tests should be confirmed by the MAT. Agglutinating antibodies can detects both IgM and IgG classes and are detectable from about days 7 to 10 after onset of symptoms.
- Advantages : It is serovar specific test. Once infected the person stays MAT positive for several years so the test is useful for epidemiological purpose.
Molecular Diagnosis
Polymerase Chain Reaction
Polymerase chain reaction will give quick results in the early stage of the disease when antibodies have not yet developed in detectable levels (<7 days)
References
- ↑ 1.0 1.1 Forbes AE, Zochowski WJ, Dubrey SW, Sivaprakasam V (2012). "Leptospirosis and Weil's disease in the UK". QJM. 105 (12): 1151–62. doi:10.1093/qjmed/hcs145. PMID 22843698.
- ↑ LastName, FirstName (2003). Human leptospirosis : guidance for diagnosis, surveillance and control. Geneva: World Health Organization. ISBN 9241545895.
- ↑ 3.0 3.1 EDWARDS GA, DOMM BM (1960). "Human leptospirosis". Medicine (Baltimore). 39: 117–56. PMID 13819407.
- ↑ Bharti AR, Nally JE, Ricaldi JN, Matthias MA, Diaz MM, Lovett MA; et al. (2003). "Leptospirosis: a zoonotic disease of global importance". Lancet Infect Dis. 3 (12): 757–71. PMID 14652202.
- ↑ 5.0 5.1 BEESON PB, HANKEY DD (1952). "Leptospiral meningitis". AMA Arch Intern Med. 89 (4): 575–83. PMID 14902167.
- ↑ CARGILL WH, BEESON PB (1947). "The value of spinal fluid examination as a diagnostic procedure in Weil's disease". Ann Intern Med. 27 (3): 396–400. PMID 20263193.
- ↑ Rule PL, Alexander AD (1986). "Gellan gum as a substitute for agar in leptospiral media". J Clin Microbiol. 23 (3): 500–4. PMC 268682. PMID 3754265.
- ↑ Bal AE, Gravekamp C, Hartskeerl RA, De Meza-Brewster J, Korver H, Terpstra WJ (1994). "Detection of leptospires in urine by PCR for early diagnosis of leptospirosis". J Clin Microbiol. 32 (8): 1894–8. PMC 263898. PMID 7989538.
- ↑ Zochowski WJ, Palmer MF, Coleman TJ (2001). "An evaluation of three commercial kits for use as screening methods for the detection of leptospiral antibodies in the UK". J Clin Pathol. 54 (1): 25–30. PMC 1731274. PMID 11271784.


{kind=link}