Duodenal atresia pathophysiology: Difference between revisions
Hamid Qazi (talk | contribs) No edit summary |
Hamid Qazi (talk | contribs) No edit summary |
||
| (One intermediate revision by the same user not shown) | |||
| Line 4: | Line 4: | ||
{{CMG}}; {{AE}} {{HQ}} | {{CMG}}; {{AE}} {{HQ}} | ||
==Overview== | ==Overview== | ||
It is thought that duodenal atresia is the result of failure of neural cell migration during the 8th to 10th week of duodenal re-canalization. It is associated with down syndrome, vertebral defects, anal anomalies, esophageal atresia, annular pancreas, malrotation, renal abnormalities, cardiac causes, and mandibulofacial anomalies. | It is thought that duodenal atresia is the result of failure of [[Nervous system|neural]] cell migration during the 8th to 10th week of [[Duodenum|duodenal]] re-canalization. It is associated with [[down syndrome]], [[Vertebra|vertebral]] defects, [[Anus|anal]] anomalies, [[esophageal atresia]], [[annular pancreas]], [[Intestinal malrotation|malrotation]], [[Kidney|renal]] abnormalities, [[cardiac]] causes, and mandibulofacial anomalies. | ||
==Pathophysiology== | ==Pathophysiology== | ||
===Pathogenesis=== | ===Pathogenesis=== | ||
*Duodenum starts developing during the 6th and 7th week of gestation.<ref name="pmid10436237">{{cite journal| author=Ando H, Kaneko K, Ito F, Seo T, Harada T, Watanabe Y| title=Embryogenesis of pancreaticobiliary maljunction inferred from development of duodenal atresia. | journal=J Hepatobiliary Pancreat Surg | year= 1999 | volume= 6 | issue= 1 | pages= 50-4 | pmid=10436237 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=10436237 }} </ref><ref name="pmid6028984">{{cite journal| author=Boyden EA, Cope JG, Bill AH| title=Anatomy and embryology of congenital intrinsic obstruction of the duodenum. | journal=Am J Surg | year= 1967 | volume= 114 | issue= 2 | pages= 190-202 | pmid=6028984 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=6028984 }} </ref> | *[[Duodenum]] starts developing during the 6th and 7th week of [[gestation]].<ref name="pmid10436237">{{cite journal| author=Ando H, Kaneko K, Ito F, Seo T, Harada T, Watanabe Y| title=Embryogenesis of pancreaticobiliary maljunction inferred from development of duodenal atresia. | journal=J Hepatobiliary Pancreat Surg | year= 1999 | volume= 6 | issue= 1 | pages= 50-4 | pmid=10436237 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=10436237 }} </ref><ref name="pmid6028984">{{cite journal| author=Boyden EA, Cope JG, Bill AH| title=Anatomy and embryology of congenital intrinsic obstruction of the duodenum. | journal=Am J Surg | year= 1967 | volume= 114 | issue= 2 | pages= 190-202 | pmid=6028984 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=6028984 }} </ref> | ||
**Re-canalization occurs during the 8th to 10th week of gestation | **Re-canalization occurs during the 8th to 10th week of [[gestation]]. | ||
*It is thought that duodenal atresia is the result of failure of re-canalization of the duodenum in 8 to 10 weeks of fetal development. | *It is thought that duodenal atresia is the result of failure of re-canalization of the [[duodenum]] in 8 to 10 weeks of [[Fetus|fetal]] development. | ||
**This is due to failure of neural cell migration | **This is due to failure of [[Neural crest|neural]] cell migration | ||
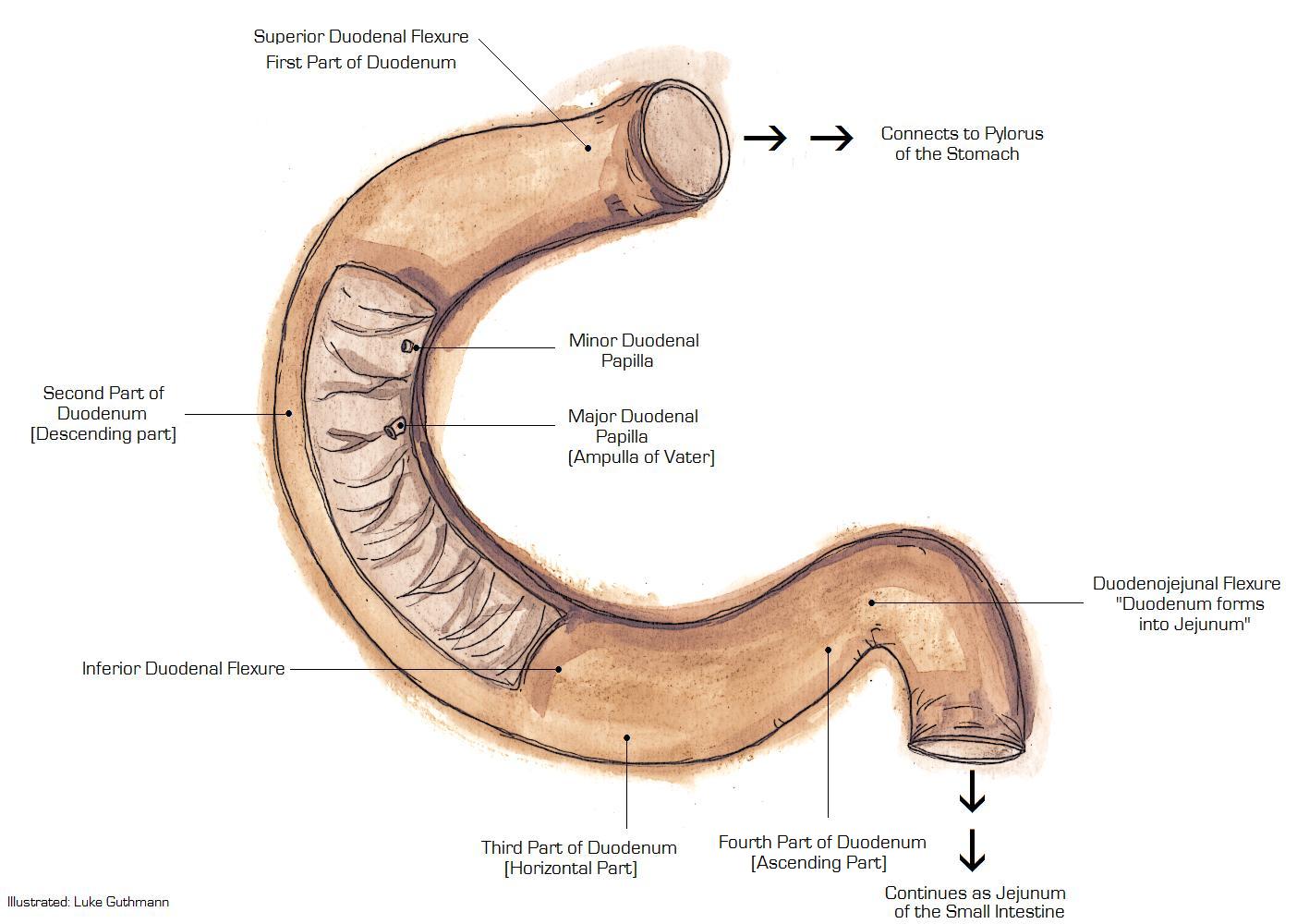
[[File:Duodenum anatomy.jpg|thumb|none|372x372px|Duodenum Anatomy.[https://www.wikidoc.org/images/0/0b/Duodenum_anatomy.jpg Source: Libre Pathology]]] | [[File:Duodenum anatomy.jpg|thumb|none|372x372px|Duodenum Anatomy.[https://www.wikidoc.org/images/0/0b/Duodenum_anatomy.jpg Source: Libre Pathology]]] | ||
| Line 18: | Line 18: | ||
==Genetics== | ==Genetics== | ||
*Duodenal atresia is not transmitted genetically. | *Duodenal atresia is not transmitted [[Genetics|genetically]]. | ||
==Associated Conditions== | ==Associated Conditions== | ||
Duodenal atresia is commonly associated with the following:<ref name="FreemanTorfs2009">{{cite journal|last1=Freeman|first1=SB|last2=Torfs|first2=CP|last3=Romitti|first3=PA|last4=Royle|first4=MH|last5=Druschel|first5=C|last6=Hobbs|first6=CA|last7=Sherman|first7=SL|title=Congenital gastrointestinal defects in Down syndrome: a report from the Atlanta and National Down Syndrome Projects|journal=Clinical Genetics|volume=75|issue=2|year=2009|pages=180–184|issn=00099163|doi=10.1111/j.1399-0004.2008.01110.x}}</ref><ref name="MorrisKennedy2016">{{cite journal|last1=Morris|first1=Grant|last2=Kennedy|first2=Alfred|last3=Cochran|first3=William|title=Small Bowel Congenital Anomalies: a Review and Update|journal=Current Gastroenterology Reports|volume=18|issue=4|year=2016|issn=1522-8037|doi=10.1007/s11894-016-0490-4}}</ref> | Duodenal atresia is commonly associated with the following:<ref name="FreemanTorfs2009">{{cite journal|last1=Freeman|first1=SB|last2=Torfs|first2=CP|last3=Romitti|first3=PA|last4=Royle|first4=MH|last5=Druschel|first5=C|last6=Hobbs|first6=CA|last7=Sherman|first7=SL|title=Congenital gastrointestinal defects in Down syndrome: a report from the Atlanta and National Down Syndrome Projects|journal=Clinical Genetics|volume=75|issue=2|year=2009|pages=180–184|issn=00099163|doi=10.1111/j.1399-0004.2008.01110.x}}</ref><ref name="MorrisKennedy2016">{{cite journal|last1=Morris|first1=Grant|last2=Kennedy|first2=Alfred|last3=Cochran|first3=William|title=Small Bowel Congenital Anomalies: a Review and Update|journal=Current Gastroenterology Reports|volume=18|issue=4|year=2016|issn=1522-8037|doi=10.1007/s11894-016-0490-4}}</ref> | ||
* Down syndrome in 25 %to 40% of cases | * [[Down syndrome]] in 25 %to 40% of cases | ||
* VATER | * VATER | ||
**Vertebral defects | **[[Vertebra|Vertebral]] defects | ||
**Anal anomalies | **[[Anus|Anal]] anomalies | ||
**Esophageal atresia | **[[Esophageal atresia]] | ||
**Renal abnormalities | **[[Kidney|Renal]] abnormalities | ||
*Malrotation | *[[Intestinal malrotation|Malrotation]] | ||
*Annular pancreas | *[[Annular pancreas]] | ||
*Biliary tract abnormalities | *[[Bile duct|Biliary]] tract abnormalities | ||
*Cardiac anomalies | *[[Heart|Cardiac]] anomalies | ||
*Mandibulofacial anomalies | *Mandibulofacial anomalies | ||
Latest revision as of 15:55, 2 January 2018
|
Duodenal Atresia Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Duodenal atresia pathophysiology On the Web |
|
American Roentgen Ray Society Images of Duodenal atresia pathophysiology |
|
Risk calculators and risk factors for Duodenal atresia pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hamid Qazi, MD, BSc [2]
Overview
It is thought that duodenal atresia is the result of failure of neural cell migration during the 8th to 10th week of duodenal re-canalization. It is associated with down syndrome, vertebral defects, anal anomalies, esophageal atresia, annular pancreas, malrotation, renal abnormalities, cardiac causes, and mandibulofacial anomalies.
Pathophysiology
Pathogenesis
- Duodenum starts developing during the 6th and 7th week of gestation.[1][2]
- Re-canalization occurs during the 8th to 10th week of gestation.
- It is thought that duodenal atresia is the result of failure of re-canalization of the duodenum in 8 to 10 weeks of fetal development.
- This is due to failure of neural cell migration

{kind=link}
Genetics
- Duodenal atresia is not transmitted genetically.
Associated Conditions
Duodenal atresia is commonly associated with the following:[3][4]
- Down syndrome in 25 %to 40% of cases
- VATER
- Vertebral defects
- Anal anomalies
- Esophageal atresia
- Renal abnormalities
- Malrotation
- Annular pancreas
- Biliary tract abnormalities
- Cardiac anomalies
- Mandibulofacial anomalies
References
- ↑ Ando H, Kaneko K, Ito F, Seo T, Harada T, Watanabe Y (1999). "Embryogenesis of pancreaticobiliary maljunction inferred from development of duodenal atresia". J Hepatobiliary Pancreat Surg. 6 (1): 50–4. PMID 10436237.
- ↑ Boyden EA, Cope JG, Bill AH (1967). "Anatomy and embryology of congenital intrinsic obstruction of the duodenum". Am J Surg. 114 (2): 190–202. PMID 6028984.
- ↑ Freeman, SB; Torfs, CP; Romitti, PA; Royle, MH; Druschel, C; Hobbs, CA; Sherman, SL (2009). "Congenital gastrointestinal defects in Down syndrome: a report from the Atlanta and National Down Syndrome Projects". Clinical Genetics. 75 (2): 180–184. doi:10.1111/j.1399-0004.2008.01110.x. ISSN 0009-9163.
- ↑ Morris, Grant; Kennedy, Alfred; Cochran, William (2016). "Small Bowel Congenital Anomalies: a Review and Update". Current Gastroenterology Reports. 18 (4). doi:10.1007/s11894-016-0490-4. ISSN 1522-8037.