Obesity cardiomyopathy: Difference between revisions
| (105 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
__NOTOC__ | __NOTOC__ | ||
[[Image:Pathophysiology OC.png|thumb|500px|'''Pathophysiology of obesity cardiomyopathy.''' Schematic is the author's own work based on "Ebong IA (2014) Mechanisms of heart failure in obesity. | [[Image:Pathophysiology OC.png|thumb|500px|'''Pathophysiology of obesity cardiomyopathy.''' Schematic is the author's own work based on "Ebong IA (2014) Mechanisms of heart failure in obesity. obesity Research and Clinical Practice 8: e540-e548.<ref name="pmid25434909" />]] | ||
{{SI}} | {{SI}} | ||
| Line 6: | Line 6: | ||
{{CMG}}; {{AE}} {{Soroush}} | {{CMG}}; {{AE}} {{Soroush}} | ||
{{SK}} | {{SK}}obesity cardiomyopathy, obesity dilated cardiomyopathy, obesity induced cardiomyopathy. | ||
==Overview== | ==Overview== | ||
Obesity cardiomyopathy is defined as congestive heart failure due to structural and [[Hemodynamics|hemodynamic]] changes because of obesity. Increased total blood volume and cardiac output because of the high metabolic activity of excessive fat in long-standing [[obesity]] may lead to left ventricular dilation, increased [[Left ventricle|left ventricular wall stress]], compensatory left ventricular hypertrophy, and | [[Obesity]] [[cardiomyopathy]] is defined as [[congestive heart failure]] due to structural and [[Hemodynamics|hemodynamic]] changes because of [[obesity]]. Increased total blood volume and [[cardiac output]] because of the high metabolic activity of excessive fat in long-standing [[obesity]] may lead to [[Cardiomegaly|left ventricular dilation]], increased [[Left ventricle|left ventricular wall stress]], compensatory [[left ventricular hypertrophy]], and l[[Diastolic dysfunction|eft ventricular diastolic dysfunction]]. Inadequate [[Hypertrophy (medical)|hypertrophy]] might tend to left ventricular [[systolic dysfunction]] due to high wall stress[[Sleep apnea|, sleep apnea]]/ [[obesity]] [[hypoventilation]] [[syndrome]] might tend to [[pulmonary hypertension]] and subsequent [[Right ventricle|right ventricul]]<nowiki/>ar structural changes. | ||
Inadequate hypertrophy might tend to left ventricular systolic dysfunction due to high wall stress | |||
My references (Temporary) | |||
<ref name="pmid17653116">{{cite journal| author=Wong C, Marwick TH| title=Obesity cardiomyopathy: pathogenesis and pathophysiology. | journal=Nat Clin Pract Cardiovasc Med | year= 2007 | volume= 4 | issue= 8 | pages= 436-43 | pmid=17653116 | doi=10.1038/ncpcardio0943 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=17653116 }} </ref> | |||
<ref name="pmid11307864">{{cite journal| author=Alpert MA| title=Obesity cardiomyopathy: pathophysiology and evolution of the clinical syndrome. | journal=Am J Med Sci | year= 2001 | volume= 321 | issue= 4 | pages= 225-36 | pmid=11307864 | doi=10.1097/00000441-200104000-00003 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=11307864 }} </ref> | |||
==Historical Perspective== | |||
<ref name=" | *[[Obesity]] [[cardiomyopathy]] is a new term, but the association between [[obesity]] and cardiac malfunction dates as far back as the late 1700s. | ||
*'''1783:''' The first mention of excess deposition of fat around the [[heart]] of obese individuals in novel literature.<ref name="pmid11307864" /> | |||
*'''1806:''' Fat tissue surrounding the heart of obese subjects was suggested as the culprit of [[heart disease]] and [[Sudden cardiac death|sudden death]] in obese patients.<ref name="pmid11307864" /> | |||
*'''late 19th Century and the early 20th Century:''' Shreds of evidence of a deleterious effect of [[obesity]] on cardiac function has appeared in the published research. | |||
*'''1933:''' the initial clinical descriptions of a pathologic [[obesity]] -associated cardiac [[morphology]] and dysfunction suggested by Saphir and Corrigan, and Smith and Willius.{{cite web |url=https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/539318 |title=ADIPOSITY OF THE HEART: A CLINICAL AND PATHOLOGIC STUDY OF ONE HUNDRED AND THIRTY-SIX OBESE PATIENTS | JAMA Internal Medicine | JAMA Network |format= |work= |accessdate=}}{{cite web |url=https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/539149 |title=FATTY INFILTRATION OF THE MYOCARDIUM | JAMA Internal Medicine | JAMA Network |format= |work= |accessdate=}} | |||
== | *'''late 20th and early 21st Century:''' Plenty of published studies revealed the cardiomyopathic processes caused by [[obesity]] and suggested that it may involve both the left and right sides of the heart, and it could occur in the absence of other cardiac or extracardiac conditions associated with [[Obesity|morbid obesity]] such as [[Hypertension|systemic hypertension]], [[diabetes mellitus]] and [[Coronary heart disease|coronary artery disease]] (CAD). <ref name="pmid3975428">{{cite journal| author=Alexander JK| title=The cardiomyopathy of obesity. | journal=Prog Cardiovasc Dis | year= 1985 | volume= 27 | issue= 5 | pages= 325-34 | pmid=3975428 | doi=10.1016/s0033-0620(85)80002-5 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=3975428 }} </ref><ref name="pmid11307864" /> | ||
Obesity | *'''[[Framingham Heart Study]]:''' FHS reported [[obesity]] is an independent [[risk factor]] for the development of [[Congestive heart failure|CHF]]. | ||
*Nevertheless, there are some authors and scientists that believe there is no such a disease, and almost every obese patients with [[cardiomyopathy]] are suffering from another disease/comorbidity of[[obesity]] .<ref name="pmid12196085">{{cite journal| author=Wilson PW, D'Agostino RB, Sullivan L, Parise H, Kannel WB| title=Overweight and obesity as determinants of cardiovascular risk: the Framingham experience. | journal=Arch Intern Med | year= 2002 | volume= 162 | issue= 16 | pages= 1867-72 | pmid=12196085 | doi=10.1001/archinte.162.16.1867 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=12196085 }} </ref> | |||
*'''[[Obesity]] as a real disorder and worldwide problem:''' | |||
*'''Ng and associates study:''' as of February 2020, their study remains the biggest and most powerful study in the [[epidemiology]] of [[obesity]]. For more than three decades '''(1980-2013)''', they recruited subjects aged between two and over 80 years old from 188 countries; the highest prevalence of [[obesity]] has been reported in Oceania, North Africa, and the Middle East, respectively which exceeded 50% of the general population. The prevalence was a little lower but still extremely high all around the world. Almost one-third of the population was [[Obesity|obese]] in North America, while in Western Europe, twenty percent of the population was [[Obesity|obese]]. This is a worldwide silent catastrophe.<ref name="pmid24880830">{{cite journal| author=Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C | display-authors=etal| title=Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. | journal=Lancet | year= 2014 | volume= 384 | issue= 9945 | pages= 766-81 | pmid=24880830 | doi=10.1016/S0140-6736(14)60460-8 | pmc=4624264 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=24880830 }} </ref> | |||
<br /> | |||
== | ==Classification== | ||
* There is no globally accepted established system for the [[classification]] of [[obesity]] [[cardiomyopathy]]. | |||
* Although it has been defined as a clinical entity for many years, "current morphological-and functional-based classification systems have excluded it as a distinct form of [[cardiomyopathy]]."<ref name="pmid26792875">{{cite journal| author=Pinto YM, Elliott PM, Arbustini E, Adler Y, Anastasakis A, Böhm M | display-authors=etal| title=Proposal for a revised definition of dilated cardiomyopathy, hypokinetic non-dilated cardiomyopathy, and its implications for clinical practice: a position statement of the ESC working group on myocardial and pericardial diseases. | journal=Eur Heart J | year= 2016 | volume= 37 | issue= 23 | pages= 1850-8 | pmid=26792875 | doi=10.1093/eurheartj/ehv727 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=26792875 }} </ref> | |||
== | * American and European cardiology societies classification contradicts in this case: | ||
The incidence/ | * The European Society of Cardiology (ESC) does not classify obesity [[cardiomyopathy]] as a type of [[Cardiomyopathy|cardiomyopathy.]] | ||
* The [[American Heart Association|American Heart Association (AHA]]) classifies [[obesity]] [[cardiomyopathy]] as a sub-type of [[dilated cardiomyopathy]] under endocrine or metabolic [[Etiology|etiologi]]<nowiki/>es of [[dilated cardiomyopathy]].<ref name="pmid27832612">{{cite journal| author=Bozkurt B, Colvin M, Cook J, Cooper LT, Deswal A, Fonarow GC | display-authors=etal| title=Current Diagnostic and Treatment Strategies for Specific Dilated Cardiomyopathies: A Scientific Statement From the American Heart Association. | journal=Circulation | year= 2016 | volume= 134 | issue= 23 | pages= e579-e646 | pmid=27832612 | doi=10.1161/CIR.0000000000000455 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=27832612 }} </ref> | |||
* The authors would like to support AHA’s classification. Nevertheless, the topic is still extremely controversial and needs further excavation. | |||
* A higher incidence of [[Dilated cardiomyopathy|idiopathic dilated cardiomyopathy]] has been reported among obese patients compared to their lean counterparts in many studies, some studies reported a direct toxic effect of [[obesity]] on [[Morphology (biology)|cardiac morphology]] and function. | |||
*There is no doubt that classification of [[obesity]] [[cardiomyopathy]] as a sub-type or an etiology of [[dilated cardiomyopathy]] might be immature. It is still controversial whether there is true [[obesity]] -induced [[cardiomyopathy]] or not? <ref name="pmid22682221">{{cite journal| author=Goldberg IJ, Trent CM, Schulze PC| title=Lipid metabolism and toxicity in the heart. | journal=Cell Metab | year= 2012 | volume= 15 | issue= 6 | pages= 805-12 | pmid=22682221 | doi=10.1016/j.cmet.2012.04.006 | pmc=3387529 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=22682221 }} </ref> | |||
*Although [[obesity]] [[cardiomyopathy]] has been developed in obese rodent models, it is still unclear whether isolated [[obesity]] can directly lead to [[cardiomyopathy]] in humans, or so-called [[obesity]] [[cardiomyopathy]] is solely the result of comorbidities of [[obesity]]. | |||
*Plenty of obese patients have a collection of concomitant and synergistic [[Risk factor|risk factors]] for developing [[Congestive heart failure|cardiac dysfunction]], [[dilated cardiomyopathy]] and [[Congestive heart failure|heart failure.]]<ref name="pmid31132859" /><ref name="pmid17653116" /> | |||
*Additionally, it is almost impossible to find a series of obese patients without hypertension, [[Lipoprotein disorders|dyslipidemia]], [[glucose intolerance]] and [[Coronary artery|coronary artery diseases]] to study. | |||
*Finally, there are some authors that believe that the term "[[obesity]] [[cardiomyopathy]]" does not exist in real world! They mentioned in their recently published article entitled '''"obesity [[cardiomyopathy]] and systolic function: [[obesity]] is not independently associated with [[dilated cardiomyopathy]]."''', that any myocardial abnormality is due to a primary co-morbidity of [[obesity]] and hence, presence of abnormal myocardial function calls for extensive studies to find out the primary reasoning behind the cardiac malfunction. They believe tha always a primary reason such as latent [[Sleep apnea|OSA]] or silent ischemia could be discovered after extensive work up.<ref name="pmid22610359">{{cite journal| author=Khan MF, Movahed MR| title=Obesity cardiomyopathy and systolic function: obesity is not independently associated with dilated cardiomyopathy. | journal=Heart Fail Rev | year= 2013 | volume= 18 | issue= 2 | pages= 207-17 | pmid=22610359 | doi=10.1007/s10741-012-9320-4 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=22610359 }} </ref> | |||
<br /> | |||
==Pathophysiology== | |||
It is thought that [[obesity]] [[cardiomyopathy]] is the result of [[Hemodynamics|hemodynamic]] changes and systemic [[Metabolism|metabolic]] changes of [[Obesity|adeposity]]. | |||
* An association between [[obesity]] and [[Congestive heart failure|heart failure]] has been shown in epidemiological studies. | |||
* Clinical studies have shown the association between [[obesity]] and [[Left ventricle|left ventricular dysfunction]], independent of [[hypertension]], [[Coronary heart disease|coronary artery disease]], and other [[Heart disease|heart diseases]]. | |||
* Experimental studies demonstrated structural and functional changes in the [[myocardium]] in response to [[obesity]]. | |||
The most important mechanisms in the development of [[obesity]] [[cardiomyopathy]] are:<ref name="pmid16376323" /><ref name="pmid27832612" /><ref name="pmid3975428" /><ref name="pmid11307864" /><ref name="pmid17653116" /><ref name="pmid25434909" /> | |||
* Metabolic disturbances ([[insulin resistance]], increased [[Fatty acid|free fatty acid]] levels, and also increased levels of [[adipokine]]<nowiki/>s), | |||
* Activation of the r[[Renin-angiotensin system|enin-angiotensin-aldosterone]] and [[sympathetic nervous system]]<nowiki/>s, | |||
* Myocardial remodeling, | |||
* Small-vessel disease (both [[Microvascular disease|microangiopathy]] and [[endothelial dysfunction]]). <ref name="pmid25434909">{{cite journal| author=Ebong IA, Goff DC, Rodriguez CJ, Chen H, Bertoni AG| title=Mechanisms of heart failure in obesity. | journal=Obes Res Clin Pract | year= 2014 | volume= 8 | issue= 6 | pages= e540-8 | pmid=25434909 | doi=10.1016/j.orcp.2013.12.005 | pmc=4250935 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=25434909 }} </ref> | |||
<br /> | |||
{| class="wikitable" | |||
|'''Mechanism''' | |||
|'''Effects/ Results''' | |||
|- | |||
| rowspan="5" |Hemodynamics | |||
|Increased blood volume | |||
|- | |||
|Increased [[stroke volume]]/Work | |||
|- | |||
|Increased [[Blood pressure|arterial pressure]] | |||
|- | |||
|Increased [[Left ventricle|LV wall stress]] | |||
|- | |||
|[[Pulmonary hypertension|Pulmonary artery hypertension]] | |||
|- | |||
| rowspan="4" |Cardiac Structure | |||
|LV concentric [[remodeling]] | |||
|- | |||
|[[Left ventricle|LV]] [[Hypertrophy (medical)|hypertrophy]] (eccentric/concentric) | |||
|- | |||
|Left atrial enlargement | |||
|- | |||
|[[Hypertrophy|RV hypertrophy]] | |||
|- | |||
| rowspan="3" |Cardiac Function | |||
|LV [[diastolic dysfunction]] | |||
|- | |||
|LV [[systolic dysfunction]] | |||
|- | |||
|RV failure | |||
|- | |||
| rowspan="2" |Inflammation | |||
|Increased [[C-reactive protein]] | |||
|- | |||
|Over-expression of [[tumor necrosis factors]] (TNF) | |||
|- | |||
| rowspan="5" |Neurohumoral | |||
|[[Insulin resistance]] and [[Hyperinsulinism|hyperinsulinemia]] | |||
|- | |||
|[[Leptin]] resistance and hyperleptinemia | |||
|- | |||
|Reduced [[adiponectin]] | |||
|- | |||
|[[Sympathetic nervous system]] over-activation | |||
|- | |||
|Activation of [[Renin-angiotensin system|renin-angiotensin-aldosterone]] system | |||
|- | |||
| rowspan="3" |Cellular | |||
|[[Hypertrophy (medical)|Hypertrophy]] | |||
|- | |||
|[[Apoptosis]] | |||
|- | |||
|[[Fibrosis]] | |||
|} | |||
==Causes== | |||
*[[Obesity]] [[cardiomyopathy]] may be caused by hemodynamic changes and systemic metabolic changes of adiposity. | |||
*[[Obesity]] itself and comorbidities of [[obesity]] such as [[hypertension]], [[diabetes]], [[Lipoprotein disorders|dyslipidemia]], [[atherosclerosis]], [[Chronic renal failure|chronic kidney disease]], [[Sleep apnea|obstructive sleep apnea]] and subsequent [[pulmonary hypertension]] are all among causes of [[obesity]] [[cardiomyopathy]]. <ref name="pmid16376323" /><ref name="pmid22682221" /><ref name="pmid26792875" /><ref name="pmid3975428" /><ref name="pmid11307864" /><ref name="pmid17653116" /><ref name="pmid25434909" /> | |||
==Differentiating obesity Cardiomyopathy from other Diseases== | |||
obesity [[cardiomyopathy]] must be differentiated from other diseases that cause [[cardiomyopathy]], such as [[hypertension]] (HTN), [[Coronary heart disease|ischemic heart disease]] (IHD), [[Pulmonary hypertension|pulmonary arterial hypertension]] (PAH), and [[Sleep apnea|obstructive sleep apnea]] (OSA).<ref name="pmid18391168" /><ref name="pmid26792875" /><ref name="pmid12196085" /><ref name="pmid11307864" /><ref name="pmid17653116" /><ref name="pmid25434909" /> | |||
==Epidemiology and Demographics== | |||
*'''Ng and associates study:''' as of February 2020, their study remains the biggest and most powerful study in the [[epidemiology]] of [[obesity]]. For more than three decades '''(1980-2013)''', they recruited subjects aged between two and over 80 years old from 188 countries; the highest prevalence of [[obesity]] has been reported in Oceania, North Africa, and the Middle East, respectively which exceeded 50% of the general population. The prevalence was a little lower but still extremely high all around the world. Almost one-third of the population was obese in North America, while in Western Europe, twenty percent of the population was obese. This is a worldwide silent catastrophe.<ref name="pmid24880830" /> | |||
*The [[prevalence]] of [[congestive heart failure]] (CHF) is approximately 2000-3000 per 100,000 individuals in industrialized countries. Around 5.7 million American adults need frequent hospitalization due to heart failure.<ref name="pmid22682221" /><ref name="pmid3975428" /><ref name="pmid11307864" /><ref name="pmid17653116" /><ref name="pmid25434909" /> | |||
*[[Obesity]] [[cardiomyopathy]] is estimated to be responsible for 11% of [[Congestive heart failure|heart failure]] cases in males and around 14% in women.<ref name="pmid11307864" /><ref name="pmid17653116" /><ref name="pmid25434909" /> | |||
==Risk Factors== | ==Risk Factors== | ||
* In morbidly obese patients, [[cardiomyopathy]] may result from [[obesity]], which may be potentiated with an increased predisposition to other [[Risk factor|risk factors]] such as [[Coronary heart disease|coronary artery disease]], [[diabetes mellitus]], [[hypertension]], [[Lipoprotein disorders|dyslipidemia]], [[insulin resistance]], [[metabolic syndrome]], [[Kidney|kidney disease,]] [[Sleep apnea|obstructive sleep apnea]], and [[Heart block|cardiac conduction abnormalities]].<ref name="pmid25434909" /><ref name="pmid26792875" /><ref name="pmid3975428" /><ref name="pmid17653116" /> | |||
==Screening== | ==Screening== | ||
*<nowiki/><nowiki/>Almost every obese patient must be [[Screening of obesity|screen]]<nowiki/>ed for [[obesity]] comorbidities which predispose them to the development of [[heart disease]] and [[obesity]] [[cardiomyopathy]] in particular. [[Screening (medicine)|Screening]] in morbid obese patients should include [[diabetes]], [[Sleep apnea|obstructive sleep apnea]] (OSA), [[hypertension]], [[Congestive heart failure|pump failure]], etc. It should be noted that history and [[physical examination]] is not appropriate in certain scenarios like [[Sleep apnea|OSA]]. A basic [[Cardiac sonographer|echocardiograph]]<nowiki/>ic study is warranted in morbidly obese patients, particularly those with comorbidities. <ref name="pmid31132859">{{cite journal| author=Robertson J, Schaufelberger M, Lindgren M, Adiels M, Schiöler L, Torén K | display-authors=etal| title=Higher Body Mass Index in Adolescence Predicts Cardiomyopathy Risk in Midlife. | journal=Circulation | year= 2019 | volume= 140 | issue= 2 | pages= 117-125 | pmid=31132859 | doi=10.1161/CIRCULATIONAHA.118.039132 | pmc=6635044 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=31132859 }} </ref><ref name="pmid17653116" /> | |||
*[[Adiponectin]] has been proposed as a [[Biomarker|biomar]]<nowiki/>[[Biomarker|ker]] that might serve as a suitable [[Screening (medicine)|screening]] test facilitating early intervention and [[Prevention (medical)|prevention]] of [[Congestive heart failure|heart failure]].<ref name="pmid17046560">{{cite journal| author=Patel DA, Srinivasan SR, Xu JH, Chen W, Berenson GS| title=Adiponectin and its correlates of cardiovascular risk in young adults: the Bogalusa Heart Study. | journal=Metabolism | year= 2006 | volume= 55 | issue= 11 | pages= 1551-7 | pmid=17046560 | doi=10.1016/j.metabol.2006.06.028 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=17046560 }} </ref> Several reports have suggested that [[leptin]] directly induced [[Hypertrophy (medical)|hypertrophy]] in both human and rodent [[Cardiac muscle|cardiomyocyte]]<nowiki/>s. <ref name="pmid16376323">{{cite journal| author=Madani S, De Girolamo S, Muñoz DM, Li RK, Sweeney G| title=Direct effects of leptin on size and extracellular matrix components of human pediatric ventricular myocytes. | journal=Cardiovasc Res | year= 2006 | volume= 69 | issue= 3 | pages= 716-25 | pmid=16376323 | doi=10.1016/j.cardiores.2005.11.022 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16376323 }} </ref> <ref name="pmid18391168">{{cite journal| author=Abel ED, Litwin SE, Sweeney G| title=Cardiac remodeling in obesity. | journal=Physiol Rev | year= 2008 | volume= 88 | issue= 2 | pages= 389-419 | pmid=18391168 | doi=10.1152/physrev.00017.2007 | pmc=2915933 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=18391168 }} </ref> | |||
==Natural History, Complications, and Prognosis== | ==Natural History, Complications, and Prognosis== | ||
If left untreated, | If left untreated, patients with [[obesity]] [[cardiomyopathy]] may progress to develop decompensated [[Congestive heart failure|heart failure]], [[Cardiac arrhythmia|arrhythmia]] and [[sudden cardiac death]]. | ||
==Diagnosis== | |||
Wong et al. described [[obesity]] [[cardiomyopathy]] very well: | |||
* ''"[[Obesity]] [[cardiomyopathy]] includes myocardial disease in obese individuals that cannot be otherwise explained by diabetes mellitus, hypertension, coronary artery disease or other etiologies. The presentation of this condition can vary from asymptomatic left ventricular (LV) dysfunction to overt [[dilated cardiomyopathy]]."'' | |||
* Hence, diagnosis of [[obesity]] cardiomyopathy calls for two steps: | |||
* 1- Diagnosis of myocardial disease, either asymptomatic LV dysfunction or overt dilated cardiomyopathy. | |||
* 2- Rolling out myocardial dysfunction secondary to [[obesity]] comorbidities such as [[diabetes mellitus]], hypertension, coronary artery disease, etc. | |||
===Diagnostic Study of Choice=== | ===Diagnostic Study of Choice=== | ||
* Imaging methods and particularly echocardiography plays the key role in diagnosis of [[obesity]] cardiomyopathy. Nevertheless magnetic resonance imaging (MRI) might be helpful as well. | |||
* Other diagnostic methods such as [[CT angiography]] or [[Angiography|conventional angiography]] might be used to role out presence of ischemia and [[Coronary heart disease|coronary disease]]. [[Nuclear medicine]] might be applied to role out micro-circulation problems. | |||
===History and Symptoms=== | |||
* The patients with [[obesity]] [[cardiomyopathy]] might be either asymptomatic, or their symptoms might misinterpret as deconditioning. | |||
The | |||
* The hallmark of [[obesity]] [[cardiomyopathy]] is sign and symptoms of pomp failure and increased function class. | |||
* Nevertheless, as mentioned before [[obesity]] [[cardiomyopathy]] is a diagnosis of exclusion and thus every other probable pathophysiology should be rolled out. Ischemic [[cardiomyopathy]], hypertension, pulmonary hypertension due to either obstructive sleep apnea or [[obesity]] hyponea are all among conditions that should be excluded. | |||
===Physical Examination=== | ===Physical Examination=== | ||
* Patients with [[obesity]] cardiomyopathy could appear normal, in mild distress or even cyanotic. | |||
* Physical examination of patients with [[obesity]] cardiomyopathy is usually remarkable for sign and symptoms of heart failure such as [[Heart sounds|S3]], [[Cardiac arrhythmia|arrhythmia]] particularly [[Atrial fibrillation|AF]], crackles in pulmonary auscultation, sacral [[edema]] or lower extremity [[edema]], JVP distension, etc. For detailed physical exam findings please refer to [[dilated cardiomyopathy physical examination]]. | |||
===Laboratory Findings=== | ===Laboratory Findings=== | ||
* '''An elevated concentration of serum [[brain natriuretic peptide]] (BNP) is diagnostic of heart failure in normal population, but in obese patients BNP levels are decreased and could be normal even in the presence of overt [[cardiomyopathy]] and [[Congestive heart failure|heart failure]].''' | |||
* In order to role out exclusion diagnoses a series of laboratory test might be used; among them are [[Arterial blood gas|ABG]], [[basic metabolic panel]] particularly lipid, and glucose levels as well [[HbA1c]], [[Cardiac marker|cardiac enzymes]], [[Thyroid-stimulating hormone|thyroid tests]], [[Biomarkers|inflammatory bio-markers]]. Not all of them, but each test or a group of them might be ordered per case. | |||
===Electrocardiogram=== | |||
* An [[The electrocardiogram|ECG]] may be helpful in the diagnosis of [[obesity]] [[cardiomyopathy]] and rolling out secondary myocardial dysfunction. | |||
* Findings on an [[The electrocardiogram|ECG]] suggestive of [[dilated cardiomyopathy]] include: | |||
* Left [[ventricular hypertrophy]] | |||
*<nowiki/>[[Atrial fibrillation]] or [[premature ventricular complex]]<nowiki/>es | |||
*Conduction delays, [[Atrioventricular block|AV nodal block]], or [[left bundle branch block|left bundle br]]<nowiki/>[[left bundle branch block|anch block]] may be observed. | |||
=== | Some studies have shown that left [[ventricular hypertrophy]], altered [[heart rate]], and anterolateral [[T wave inversion|T-wave inversion]] can [[Prediction|predict]] the risk of [[Mortality rate|mortality]] or [[heart transplantation]] in [[dilated cardiomyopathy]] patients.<ref name="pmid30985353">{{cite journal| author=Merlo M, Zaffalon D, Stolfo D, Altinier A, Barbati G, Zecchin M et al.| title=ECG in dilated cardiomyopathy: specific findings and long-term prognostic significance. | journal=J Cardiovasc Med (Hagerstown) | year= 2019 | volume= 20 | issue= 7 | pages= 450-458 | pmid=30985353 | doi=10.2459/JCM.0000000000000804 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=30985353 }}</ref><ref name="pmid7815010">{{cite journal| author=Momiyama Y, Mitamura H, Kimura M| title=ECG characteristics of dilated cardiomyopathy. | journal=J Electrocardiol | year= 1994 | volume= 27 | issue= 4 | pages= 323-8 | pmid=7815010 | doi=10.1016/s0022-0736(05)80270-5 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=7815010 }}</ref> | ||
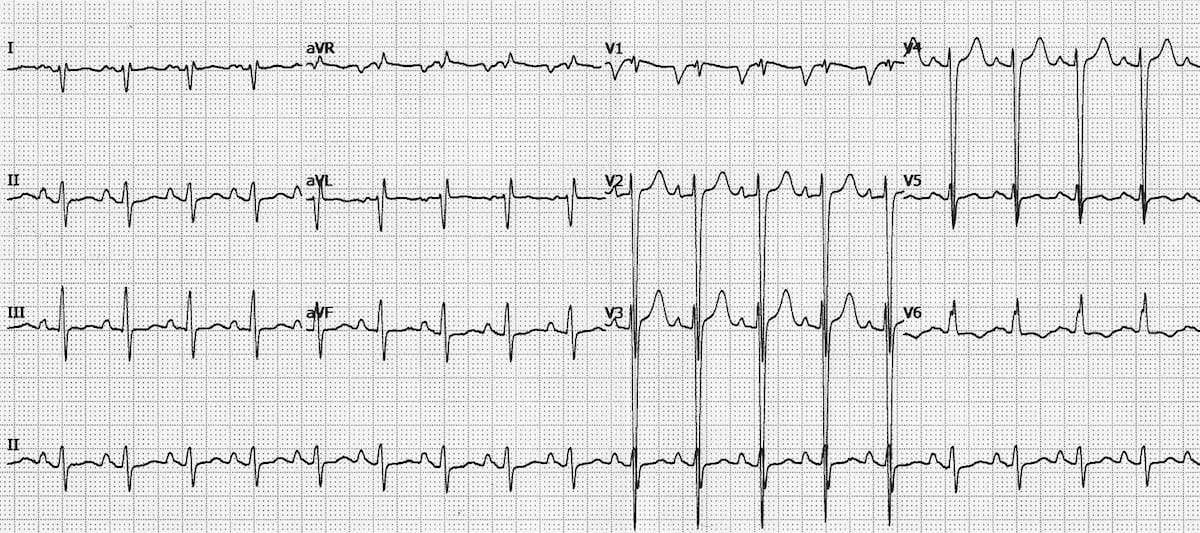
There | [[Image:ECG-Ischaemic-dilated-cardiomyopathy-1.jpg|left|400px|thumb|There is marked LVH (S wave in V2 > 35 mm) with dominant S waves in V1-4. There is evidence of right axis deviation, left atrial enlargement, and peaked p waves in lead II. Case courtesy of Dr Ed Burns <ref>https://litfl.com/wp-content/uploads/2018/08/ECG-Ischaemic-dilated-cardiomyopathy-1.jpg</ref>]] | ||
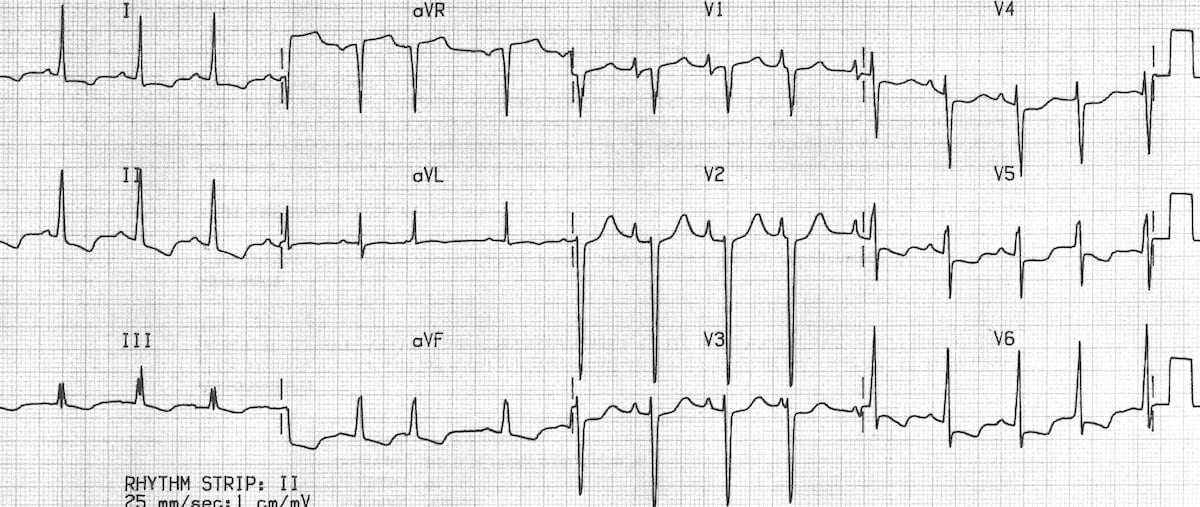
[[Image:ECG-Idiopathic-dilated-cardiomyopathy-Biatrial-hypertrophy.jpg|center|400 px|thumb|Left ventricular hypertrophy with large precordial voltages and an LV strain pattern in leads with a dominant R wave (I, II, V6). There is also evidence of biatrial enlargement in V1. Case Courtsy of Dr Ed Burns. <ref>https://litfl.com/wp-content/uploads/2018/08/ECG-Idiopathic-dilated-cardiomyopathy-Biatrial-hypertrophy.jpg</ref>]] | |||
<br /> | |||
* '''It should be noted that "Although the QTc may not be extremely increased (≈440 ms) in the obese population, it is important to emphasize that screening for prolonged QT in [[obesity]] may have stringent criteria because a prolongation of QTc of >420 ms may be predictive of increased mortality rates in a healthy population followed up for 15 years." <ref name="pmid1914093">{{cite journal| author=Schouten EG, Dekker JM, Meppelink P, Kok FJ, Vandenbroucke JP, Pool J| title=QT interval prolongation predicts cardiovascular mortality in an apparently healthy population. | journal=Circulation | year= 1991 | volume= 84 | issue= 4 | pages= 1516-23 | pmid=1914093 | doi=10.1161/01.cir.84.4.1516 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=1914093 }} </ref><ref name="pmid16380542">{{cite journal| author=Poirier P, Giles TD, Bray GA, Hong Y, Stern JS, Pi-Sunyer FX | display-authors=etal| title=Obesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight loss: an update of the 1997 American Heart Association Scientific Statement on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. | journal=Circulation | year= 2006 | volume= 113 | issue= 6 | pages= 898-918 | pmid=16380542 | doi=10.1161/CIRCULATIONAHA.106.171016 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16380542 }} </ref>''' | |||
===X-ray=== | ===X-ray=== | ||
An x-ray may be helpful in the diagnosis of [[obesity]] cardiomyopathy. Findings on an x-ray suggestive of [[obesity]] cardiomyopathy include: | |||
* Enlarged [[left ventricle]] and [[Atrium (heart)|atria]] | |||
* [[Pulmonary edema]]: [[Pulmonary vascular congestion]] increases the risk of acute decompensated [[Congestive heart failure|heart failure]] by about 12 folds. | |||
* Associated [[Pleural effusion|pleural effusions]].<ref name="pmid2225878">{{cite journal| author=Richter C, Richter K, Boewer V| title=Significant X-ray patterns in cardiomyopathy--an approach improving noninvasive diagnosis. | journal=Cor Vasa | year= 1990 | volume= 32 | issue= 4 | pages= 290-301 | pmid=2225878 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=2225878 }}</ref> | |||
[[Chest X-ray]] may give clues to the cause of DCM as [[congenital malformations]], valve [[calcification]], or evidence of [[trauma]] ([[Alcoholism|alcoholic]] patients) | |||
<br />[[File:DifDilatedCardiomyoMagCXR.png|center|thumb|A Chest x-ray of dilated cardiomyopathy, showing enlargement of the cardiac chambers, particularly the cardiac ventricles. Courtesy of James Heilman, MD<ref>https://commons.wikimedia.org/wiki/File:DifDilatedCardiomyoMagCXR.png/</ref>]] | |||
<br /> | |||
===Echocardiography or Ultrasound=== | ===Echocardiography or Ultrasound=== | ||
*Echocardiography is the main diagnostic tool in the diagnosis of [[obesity]] cardiomyopathy. Findings on an echocardiography diagnostic of [[obesity]] [[cardiomyopathy]] include LV dysfunction, decreased [[ejection fraction]], dilated heart chambers, wall motion abnormalities, secondary valvular abnormalities, etc. | |||
*In the presence of overt [[dilated cardiomyopathy]] the followings might be present: | |||
'''Overt dilated Cardiomyopathy''' | |||
*Echocardiographic findings of [[dilated cardiomyopathy]] include:<ref name="pmid19889654">{{cite journal| author=Thomas DE, Wheeler R, Yousef ZR, Masani ND| title=The role of echocardiography in guiding management in dilated cardiomyopathy. | journal=Eur J Echocardiogr | year= 2009 | volume= 10 | issue= 8 | pages= iii15-21 | pmid=19889654 | doi=10.1093/ejechocard/jep158 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=19889654 }}</ref><ref name="pmid28592613">{{cite journal| author=Mathew T, Williams L, Navaratnam G, Rana B, Wheeler R, Collins K et al.| title=Diagnosis and assessment of dilated cardiomyopathy: a guideline protocol from the British Society of Echocardiography. | journal=Echo Res Pract | year= 2017 | volume= 4 | issue= 2 | pages= G1-G13 | pmid=28592613 | doi=10.1530/ERP-16-0037 | pmc=5574280 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=28592613 }}</ref> | |||
:*Dilation of the [[left ventricle]]; however, may include dilatation of all 4 [[cardiac chambers|cardiac chambers.]] | |||
:*Left ventricular wall thickness usually is normal, but the dilation of the LV mass is increased. | |||
:*In addition, there is a global reduction in systolic function. | |||
:*Occasionally there may also be focal wall motion abnormalities even in patients without flow-limiting [[coronary artery disease]]. | |||
*The diagnosis requires a dilated [[left ventricle]] and low [[ejection fraction]]. | |||
{{#ev:youtube|ou3a7Htbrvw}} | |||
===CT scan=== | ===CT scan=== | ||
There are no CT | There are no specific CT findings exclusively for obesity cardiomyopathy but, | ||
*Cardiac CT scan and CT angiography may be helpful in the diagnosis of obesity cardiomyopathy and excluding the other disorders that might present similar to obesity cardiomyopathy. Findings on CT scan suggestive of obesity cardiomyopathy include: | |||
*Increased (Single/bi)ventricular volume and decreased [[ejection fraction]] '''(Please notein the presence of volvular regurgitation EF interpretation is different, even a normal EF is considered abnormal in a patients with MR, indeed EF lower than 60 percent are considered abnormal.)''' | |||
* Assessing the regional wall motion (with cine-loop formatting).<ref name="pmid16188534">{{cite journal| author=Lessick J, Mutlak D, Rispler S, Ghersin E, Dragu R, Litmanovich D et al.| title=Comparison of multidetector computed tomography versus echocardiography for assessing regional left ventricular function. | journal=Am J Cardiol | year= 2005 | volume= 96 | issue= 7 | pages= 1011-5 | pmid=16188534 | doi=10.1016/j.amjcard.2005.05.062 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16188534 }}</ref> | |||
*'''Excluding [[ischemia]]''': (Cardiac [[CT angiography|CTA]] has a 98% diagnostic [[Sensitivity (tests)|sensitivity]] and 97% [[Specificity (tests)|specificity]] in excluding [[ischemic cardiomyopathy]]). Also, [[Myocardial perfusion scan|Myocardial perfusion analysis]] of the [[coronary arteries]] is also beneficial.<ref name="pmid21328027">{{cite journal| author=Bhatti S, Hakeem A, Yousuf MA, Al-Khalidi HR, Mazur W, Shizukuda Y| title=Diagnostic performance of computed tomography angiography for differentiating ischemic vs nonischemic cardiomyopathy. | journal=J Nucl Cardiol | year= 2011 | volume= 18 | issue= 3 | pages= 407-20 | pmid=21328027 | doi=10.1007/s12350-011-9346-3 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=21328027 }}</ref> | |||
* Differential diagnosis of [[Dilated cardiomyopathy|DCM]] from [[hypertrophic cardiomyopathy]], arrhythmogenic right ventricular dysplasia, and left ventricular [[Noncompaction cardiomyopathy|noncompaction]].<ref name="pmid26033904">{{cite journal| author=Levine A, Hecht HS| title=Cardiac CT Angiography in Congestive Heart Failure. | journal=J Nucl Med | year= 2015 | volume= 56 Suppl 4 | issue= | pages= 46S-51S | pmid=26033904 | doi=10.2967/jnumed.114.150441 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=26033904 }}</ref> | |||
[[Image:DifCardioMag.png|center|400px|thumb|Cardiac CT scan showing enlarged cardiac chambers, in particular dilated ventricles. Case Courtesy: James Heliman, MD<ref>https://upload.wikimedia.org/wikipedia/commons/3/34/DifCardioMag.png/</ref>]] | |||
<br /> | |||
===MRI=== | ===MRI=== | ||
* There are no specific MRI findings exclusively for [[obesity]] cardiomyopathy but, | |||
*cardiac magnetic resonance imaging (MRI) might be helpful in diagnosis of dilated cardiomyopathy, studying fibrosis and inflammation and finding the etiology of the dilated cardiomyopathy. | |||
====ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance<ref name="pmid20479157">{{cite journal| author=American College of Cardiology Foundation Task Force on Expert Consensus Documents. Hundley WG, Bluemke DA, Finn JP, Flamm SD, Fogel MA et al.| title=ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. | journal=Circulation | year= 2010 | volume= 121 | issue= 22 | pages= 2462-508 | pmid=20479157 | doi=10.1161/CIR.0b013e3181d44a8f | pmc=PMC3034132 | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=20479157 }} </ref> (DO NOT EDIT)==== | |||
{{cquote| | |||
CMR may be used for assessment of patients with LV dysfunction or hypertrophy or suspected forms of cardiac injury not related to | |||
ischemic heart disease. When the diagnosis is unclear, CMR may be considered to identify the etiology of cardiac dysfunction in | |||
patients presenting with heart failure, including | |||
*Evaluation of dilated cardiomyopathy in the setting of normal coronary arteries, | |||
*Patients with positive cardiac enzymes without obstructive [[atherosclerosis]] on [[angiography]], | |||
*Patients suspected of [[amyloidosis]] or other infiltrative diseases, | |||
*[[Hypertrophic cardiomyopathy]], | |||
*[[Arrhythmogenic right ventricular dysplasia]], or | |||
*[[Syncope]] or [[ventricular arrhythmia]]. | |||
}} | |||
===Other Imaging Findings=== | ===Other Imaging Findings=== | ||
* Conventional [[cardiac catheterization]] and [[Angiogram|angiography]] plays the key role in diagnosis and management of [[Coronary heart disease|ischemic heart disease]] and certain valvular abnormalities. | |||
* Nuclear medicine might be applied to study microcirculation. | |||
===Other Diagnostic Studies=== | ===Other Diagnostic Studies=== | ||
* Conventional [[cardiac catheterization]] and [[Angiogram|angiography]] plays the key role in diagnosis and management of [[Coronary heart disease|ischemic heart disease]] and certain valvular abnormalities. | |||
*[[Genetics|Genetic]] tests are warranted in selected patients with [[dilated cardiomyopathy]]. | |||
[ | *[[Polysomnography]] might be helpful in diagnosis and management of [[Sleep apnea|obstructive sleep apnea]] in morbidly obese patients. | ||
* Endomyocardial [[biopsy]] is no longer recommended in studying dilated cardiomyopathy. | |||
==Treatment== | ==Treatment== | ||
===Medical Therapy=== | ===Medical Therapy=== | ||
The mainstay of treatment for [[obesity]] [[cardiomyopathy]] is weight loss and management of comorbidities of obesity such as [[hypertension]] and [[Sleep apnea|obstructive sleep apnea]]. | |||
The mainstay of treatment for | |||
===Surgery=== | ===Surgery=== | ||
Surgical intervention is not recommended for the management of obesity cardiomyopathy. | Surgical intervention is not recommended for the management of [[obesity]] [[cardiomyopathy]]. | ||
The exception is [[bariatric surgery]] which is indicated in morbidly obese patients with [[Body mass index|BMI]] more than 40 , or [[Body mass index|BMI]] more than 35 with comorbiditioes. | |||
===Primary Prevention=== | ===Primary Prevention=== | ||
Effective measures for the p[[Primary prevention|rimary prevention]] of [[obesity]] [[cardiomyopathy]] include weight loss and management of comorbidities of [[obesity]] such as [[hypertension]] and [[Sleep apnea|obstructive sleep apnea]]. | |||
===Secondary Prevention=== | ===Secondary Prevention=== | ||
Effective measures for the secondary prevention of [[obesity]] [[cardiomyopathy]] include management of heat failure, placement of [[Implantable cardioverter defibrillator|ICD]] or [[Artificial pacemaker|pacemaker]] when indicated as well as weight loss and management of comorbidities of [[obesity]] such as [[hypertension]] and [[Sleep apnea|obstructive sleep apnea]].. | |||
Effective measures for the secondary prevention of obesity cardiomyopathy include [ | |||
==References== | ==References== | ||
Latest revision as of 14:50, 28 February 2020

Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Soroush Seifirad, M.D.[2]
Synonyms and keywords:obesity cardiomyopathy, obesity dilated cardiomyopathy, obesity induced cardiomyopathy.
Overview
Obesity cardiomyopathy is defined as congestive heart failure due to structural and hemodynamic changes because of obesity. Increased total blood volume and cardiac output because of the high metabolic activity of excessive fat in long-standing obesity may lead to left ventricular dilation, increased left ventricular wall stress, compensatory left ventricular hypertrophy, and left ventricular diastolic dysfunction. Inadequate hypertrophy might tend to left ventricular systolic dysfunction due to high wall stress, sleep apnea/ obesity hypoventilation syndrome might tend to pulmonary hypertension and subsequent right ventricular structural changes.
My references (Temporary)
Historical Perspective
- Obesity cardiomyopathy is a new term, but the association between obesity and cardiac malfunction dates as far back as the late 1700s.
- 1783: The first mention of excess deposition of fat around the heart of obese individuals in novel literature.[3]
- 1806: Fat tissue surrounding the heart of obese subjects was suggested as the culprit of heart disease and sudden death in obese patients.[3]
- late 19th Century and the early 20th Century: Shreds of evidence of a deleterious effect of obesity on cardiac function has appeared in the published research.
- 1933: the initial clinical descriptions of a pathologic obesity -associated cardiac morphology and dysfunction suggested by Saphir and Corrigan, and Smith and Willius."ADIPOSITY OF THE HEART: A CLINICAL AND PATHOLOGIC STUDY OF ONE HUNDRED AND THIRTY-SIX OBESE PATIENTS | JAMA Internal Medicine | JAMA Network"."FATTY INFILTRATION OF THE MYOCARDIUM | JAMA Internal Medicine | JAMA Network".
- late 20th and early 21st Century: Plenty of published studies revealed the cardiomyopathic processes caused by obesity and suggested that it may involve both the left and right sides of the heart, and it could occur in the absence of other cardiac or extracardiac conditions associated with morbid obesity such as systemic hypertension, diabetes mellitus and coronary artery disease (CAD). [4][3]
- Framingham Heart Study: FHS reported obesity is an independent risk factor for the development of CHF.
- Nevertheless, there are some authors and scientists that believe there is no such a disease, and almost every obese patients with cardiomyopathy are suffering from another disease/comorbidity ofobesity .[5]
- Obesity as a real disorder and worldwide problem:
- Ng and associates study: as of February 2020, their study remains the biggest and most powerful study in the epidemiology of obesity. For more than three decades (1980-2013), they recruited subjects aged between two and over 80 years old from 188 countries; the highest prevalence of obesity has been reported in Oceania, North Africa, and the Middle East, respectively which exceeded 50% of the general population. The prevalence was a little lower but still extremely high all around the world. Almost one-third of the population was obese in North America, while in Western Europe, twenty percent of the population was obese. This is a worldwide silent catastrophe.[6]
Classification
- There is no globally accepted established system for the classification of obesity cardiomyopathy.
- Although it has been defined as a clinical entity for many years, "current morphological-and functional-based classification systems have excluded it as a distinct form of cardiomyopathy."[7]
- American and European cardiology societies classification contradicts in this case:
- The European Society of Cardiology (ESC) does not classify obesity cardiomyopathy as a type of cardiomyopathy.
- The American Heart Association (AHA) classifies obesity cardiomyopathy as a sub-type of dilated cardiomyopathy under endocrine or metabolic etiologies of dilated cardiomyopathy.[8]
- The authors would like to support AHA’s classification. Nevertheless, the topic is still extremely controversial and needs further excavation.
- A higher incidence of idiopathic dilated cardiomyopathy has been reported among obese patients compared to their lean counterparts in many studies, some studies reported a direct toxic effect of obesity on cardiac morphology and function.
- There is no doubt that classification of obesity cardiomyopathy as a sub-type or an etiology of dilated cardiomyopathy might be immature. It is still controversial whether there is true obesity -induced cardiomyopathy or not? [9]
- Although obesity cardiomyopathy has been developed in obese rodent models, it is still unclear whether isolated obesity can directly lead to cardiomyopathy in humans, or so-called obesity cardiomyopathy is solely the result of comorbidities of obesity.
- Plenty of obese patients have a collection of concomitant and synergistic risk factors for developing cardiac dysfunction, dilated cardiomyopathy and heart failure.[10][2]
- Additionally, it is almost impossible to find a series of obese patients without hypertension, dyslipidemia, glucose intolerance and coronary artery diseases to study.
- Finally, there are some authors that believe that the term "obesity cardiomyopathy" does not exist in real world! They mentioned in their recently published article entitled "obesity cardiomyopathy and systolic function: obesity is not independently associated with dilated cardiomyopathy.", that any myocardial abnormality is due to a primary co-morbidity of obesity and hence, presence of abnormal myocardial function calls for extensive studies to find out the primary reasoning behind the cardiac malfunction. They believe tha always a primary reason such as latent OSA or silent ischemia could be discovered after extensive work up.[11]
Pathophysiology
It is thought that obesity cardiomyopathy is the result of hemodynamic changes and systemic metabolic changes of adeposity.
- An association between obesity and heart failure has been shown in epidemiological studies.
- Clinical studies have shown the association between obesity and left ventricular dysfunction, independent of hypertension, coronary artery disease, and other heart diseases.
- Experimental studies demonstrated structural and functional changes in the myocardium in response to obesity.
The most important mechanisms in the development of obesity cardiomyopathy are:[12][8][4][3][2][1]
- Metabolic disturbances (insulin resistance, increased free fatty acid levels, and also increased levels of adipokines),
- Activation of the renin-angiotensin-aldosterone and sympathetic nervous systems,
- Myocardial remodeling,
- Small-vessel disease (both microangiopathy and endothelial dysfunction). [1]
| Mechanism | Effects/ Results |
| Hemodynamics | Increased blood volume |
| Increased stroke volume/Work | |
| Increased arterial pressure | |
| Increased LV wall stress | |
| Pulmonary artery hypertension | |
| Cardiac Structure | LV concentric remodeling |
| LV hypertrophy (eccentric/concentric) | |
| Left atrial enlargement | |
| RV hypertrophy | |
| Cardiac Function | LV diastolic dysfunction |
| LV systolic dysfunction | |
| RV failure | |
| Inflammation | Increased C-reactive protein |
| Over-expression of tumor necrosis factors (TNF) | |
| Neurohumoral | Insulin resistance and hyperinsulinemia |
| Leptin resistance and hyperleptinemia | |
| Reduced adiponectin | |
| Sympathetic nervous system over-activation | |
| Activation of renin-angiotensin-aldosterone system | |
| Cellular | Hypertrophy |
| Apoptosis | |
| Fibrosis |
Causes
- Obesity cardiomyopathy may be caused by hemodynamic changes and systemic metabolic changes of adiposity.
- Obesity itself and comorbidities of obesity such as hypertension, diabetes, dyslipidemia, atherosclerosis, chronic kidney disease, obstructive sleep apnea and subsequent pulmonary hypertension are all among causes of obesity cardiomyopathy. [12][9][7][4][3][2][1]
Differentiating obesity Cardiomyopathy from other Diseases
obesity cardiomyopathy must be differentiated from other diseases that cause cardiomyopathy, such as hypertension (HTN), ischemic heart disease (IHD), pulmonary arterial hypertension (PAH), and obstructive sleep apnea (OSA).[13][7][5][3][2][1]
Epidemiology and Demographics
- Ng and associates study: as of February 2020, their study remains the biggest and most powerful study in the epidemiology of obesity. For more than three decades (1980-2013), they recruited subjects aged between two and over 80 years old from 188 countries; the highest prevalence of obesity has been reported in Oceania, North Africa, and the Middle East, respectively which exceeded 50% of the general population. The prevalence was a little lower but still extremely high all around the world. Almost one-third of the population was obese in North America, while in Western Europe, twenty percent of the population was obese. This is a worldwide silent catastrophe.[6]
- The prevalence of congestive heart failure (CHF) is approximately 2000-3000 per 100,000 individuals in industrialized countries. Around 5.7 million American adults need frequent hospitalization due to heart failure.[9][4][3][2][1]
- Obesity cardiomyopathy is estimated to be responsible for 11% of heart failure cases in males and around 14% in women.[3][2][1]
Risk Factors
- In morbidly obese patients, cardiomyopathy may result from obesity, which may be potentiated with an increased predisposition to other risk factors such as coronary artery disease, diabetes mellitus, hypertension, dyslipidemia, insulin resistance, metabolic syndrome, kidney disease, obstructive sleep apnea, and cardiac conduction abnormalities.[1][7][4][2]
Screening
- Almost every obese patient must be screened for obesity comorbidities which predispose them to the development of heart disease and obesity cardiomyopathy in particular. Screening in morbid obese patients should include diabetes, obstructive sleep apnea (OSA), hypertension, pump failure, etc. It should be noted that history and physical examination is not appropriate in certain scenarios like OSA. A basic echocardiographic study is warranted in morbidly obese patients, particularly those with comorbidities. [10][2]
- Adiponectin has been proposed as a biomarker that might serve as a suitable screening test facilitating early intervention and prevention of heart failure.[14] Several reports have suggested that leptin directly induced hypertrophy in both human and rodent cardiomyocytes. [12] [13]
Natural History, Complications, and Prognosis
If left untreated, patients with obesity cardiomyopathy may progress to develop decompensated heart failure, arrhythmia and sudden cardiac death.
Diagnosis
Wong et al. described obesity cardiomyopathy very well:
- "Obesity cardiomyopathy includes myocardial disease in obese individuals that cannot be otherwise explained by diabetes mellitus, hypertension, coronary artery disease or other etiologies. The presentation of this condition can vary from asymptomatic left ventricular (LV) dysfunction to overt dilated cardiomyopathy."
- Hence, diagnosis of obesity cardiomyopathy calls for two steps:
- 1- Diagnosis of myocardial disease, either asymptomatic LV dysfunction or overt dilated cardiomyopathy.
- 2- Rolling out myocardial dysfunction secondary to obesity comorbidities such as diabetes mellitus, hypertension, coronary artery disease, etc.
Diagnostic Study of Choice
- Imaging methods and particularly echocardiography plays the key role in diagnosis of obesity cardiomyopathy. Nevertheless magnetic resonance imaging (MRI) might be helpful as well.
- Other diagnostic methods such as CT angiography or conventional angiography might be used to role out presence of ischemia and coronary disease. Nuclear medicine might be applied to role out micro-circulation problems.
History and Symptoms
- The patients with obesity cardiomyopathy might be either asymptomatic, or their symptoms might misinterpret as deconditioning.
- The hallmark of obesity cardiomyopathy is sign and symptoms of pomp failure and increased function class.
- Nevertheless, as mentioned before obesity cardiomyopathy is a diagnosis of exclusion and thus every other probable pathophysiology should be rolled out. Ischemic cardiomyopathy, hypertension, pulmonary hypertension due to either obstructive sleep apnea or obesity hyponea are all among conditions that should be excluded.
Physical Examination
- Patients with obesity cardiomyopathy could appear normal, in mild distress or even cyanotic.
- Physical examination of patients with obesity cardiomyopathy is usually remarkable for sign and symptoms of heart failure such as S3, arrhythmia particularly AF, crackles in pulmonary auscultation, sacral edema or lower extremity edema, JVP distension, etc. For detailed physical exam findings please refer to dilated cardiomyopathy physical examination.
Laboratory Findings
- An elevated concentration of serum brain natriuretic peptide (BNP) is diagnostic of heart failure in normal population, but in obese patients BNP levels are decreased and could be normal even in the presence of overt cardiomyopathy and heart failure.
- In order to role out exclusion diagnoses a series of laboratory test might be used; among them are ABG, basic metabolic panel particularly lipid, and glucose levels as well HbA1c, cardiac enzymes, thyroid tests, inflammatory bio-markers. Not all of them, but each test or a group of them might be ordered per case.
Electrocardiogram
- An ECG may be helpful in the diagnosis of obesity cardiomyopathy and rolling out secondary myocardial dysfunction.
- Findings on an ECG suggestive of dilated cardiomyopathy include:
- Left ventricular hypertrophy
- Atrial fibrillation or premature ventricular complexes
- Conduction delays, AV nodal block, or left bundle branch block may be observed.
Some studies have shown that left ventricular hypertrophy, altered heart rate, and anterolateral T-wave inversion can predict the risk of mortality or heart transplantation in dilated cardiomyopathy patients.[15][16]


- It should be noted that "Although the QTc may not be extremely increased (≈440 ms) in the obese population, it is important to emphasize that screening for prolonged QT in obesity may have stringent criteria because a prolongation of QTc of >420 ms may be predictive of increased mortality rates in a healthy population followed up for 15 years." [19][20]
X-ray
An x-ray may be helpful in the diagnosis of obesity cardiomyopathy. Findings on an x-ray suggestive of obesity cardiomyopathy include:
- Enlarged left ventricle and atria
- Pulmonary edema: Pulmonary vascular congestion increases the risk of acute decompensated heart failure by about 12 folds.
- Associated pleural effusions.[21]
Chest X-ray may give clues to the cause of DCM as congenital malformations, valve calcification, or evidence of trauma (alcoholic patients)

Echocardiography or Ultrasound
- Echocardiography is the main diagnostic tool in the diagnosis of obesity cardiomyopathy. Findings on an echocardiography diagnostic of obesity cardiomyopathy include LV dysfunction, decreased ejection fraction, dilated heart chambers, wall motion abnormalities, secondary valvular abnormalities, etc.
- In the presence of overt dilated cardiomyopathy the followings might be present:
Overt dilated Cardiomyopathy
- Echocardiographic findings of dilated cardiomyopathy include:[23][24]
- Dilation of the left ventricle; however, may include dilatation of all 4 cardiac chambers.
- Left ventricular wall thickness usually is normal, but the dilation of the LV mass is increased.
- In addition, there is a global reduction in systolic function.
- Occasionally there may also be focal wall motion abnormalities even in patients without flow-limiting coronary artery disease.
- The diagnosis requires a dilated left ventricle and low ejection fraction.
{{#ev:youtube|ou3a7Htbrvw}}
CT scan
There are no specific CT findings exclusively for obesity cardiomyopathy but,
- Cardiac CT scan and CT angiography may be helpful in the diagnosis of obesity cardiomyopathy and excluding the other disorders that might present similar to obesity cardiomyopathy. Findings on CT scan suggestive of obesity cardiomyopathy include:
- Increased (Single/bi)ventricular volume and decreased ejection fraction (Please notein the presence of volvular regurgitation EF interpretation is different, even a normal EF is considered abnormal in a patients with MR, indeed EF lower than 60 percent are considered abnormal.)
- Assessing the regional wall motion (with cine-loop formatting).[25]
- Excluding ischemia: (Cardiac CTA has a 98% diagnostic sensitivity and 97% specificity in excluding ischemic cardiomyopathy). Also, Myocardial perfusion analysis of the coronary arteries is also beneficial.[26]
- Differential diagnosis of DCM from hypertrophic cardiomyopathy, arrhythmogenic right ventricular dysplasia, and left ventricular noncompaction.[27]

MRI
- There are no specific MRI findings exclusively for obesity cardiomyopathy but,
- cardiac magnetic resonance imaging (MRI) might be helpful in diagnosis of dilated cardiomyopathy, studying fibrosis and inflammation and finding the etiology of the dilated cardiomyopathy.
ACC/AHA Guidelines- ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance[29] (DO NOT EDIT)
| “ |
CMR may be used for assessment of patients with LV dysfunction or hypertrophy or suspected forms of cardiac injury not related to ischemic heart disease. When the diagnosis is unclear, CMR may be considered to identify the etiology of cardiac dysfunction in patients presenting with heart failure, including
|
” |
Other Imaging Findings
- Conventional cardiac catheterization and angiography plays the key role in diagnosis and management of ischemic heart disease and certain valvular abnormalities.
- Nuclear medicine might be applied to study microcirculation.
Other Diagnostic Studies
- Conventional cardiac catheterization and angiography plays the key role in diagnosis and management of ischemic heart disease and certain valvular abnormalities.
- Genetic tests are warranted in selected patients with dilated cardiomyopathy.
- Polysomnography might be helpful in diagnosis and management of obstructive sleep apnea in morbidly obese patients.
- Endomyocardial biopsy is no longer recommended in studying dilated cardiomyopathy.
Treatment
Medical Therapy
The mainstay of treatment for obesity cardiomyopathy is weight loss and management of comorbidities of obesity such as hypertension and obstructive sleep apnea.
Surgery
Surgical intervention is not recommended for the management of obesity cardiomyopathy.
The exception is bariatric surgery which is indicated in morbidly obese patients with BMI more than 40 , or BMI more than 35 with comorbiditioes.
Primary Prevention
Effective measures for the primary prevention of obesity cardiomyopathy include weight loss and management of comorbidities of obesity such as hypertension and obstructive sleep apnea.
Secondary Prevention
Effective measures for the secondary prevention of obesity cardiomyopathy include management of heat failure, placement of ICD or pacemaker when indicated as well as weight loss and management of comorbidities of obesity such as hypertension and obstructive sleep apnea..
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 Ebong IA, Goff DC, Rodriguez CJ, Chen H, Bertoni AG (2014). "Mechanisms of heart failure in obesity". Obes Res Clin Pract. 8 (6): e540–8. doi:10.1016/j.orcp.2013.12.005. PMC 4250935. PMID 25434909.
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 2.6 2.7 2.8 Wong C, Marwick TH (2007). "Obesity cardiomyopathy: pathogenesis and pathophysiology". Nat Clin Pract Cardiovasc Med. 4 (8): 436–43. doi:10.1038/ncpcardio0943. PMID 17653116.
- ↑ 3.0 3.1 3.2 3.3 3.4 3.5 3.6 3.7 3.8 Alpert MA (2001). "Obesity cardiomyopathy: pathophysiology and evolution of the clinical syndrome". Am J Med Sci. 321 (4): 225–36. doi:10.1097/00000441-200104000-00003. PMID 11307864.
- ↑ 4.0 4.1 4.2 4.3 4.4 Alexander JK (1985). "The cardiomyopathy of obesity". Prog Cardiovasc Dis. 27 (5): 325–34. doi:10.1016/s0033-0620(85)80002-5. PMID 3975428.
- ↑ 5.0 5.1 Wilson PW, D'Agostino RB, Sullivan L, Parise H, Kannel WB (2002). "Overweight and obesity as determinants of cardiovascular risk: the Framingham experience". Arch Intern Med. 162 (16): 1867–72. doi:10.1001/archinte.162.16.1867. PMID 12196085.
- ↑ 6.0 6.1 Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C; et al. (2014). "Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013". Lancet. 384 (9945): 766–81. doi:10.1016/S0140-6736(14)60460-8. PMC 4624264. PMID 24880830.
- ↑ 7.0 7.1 7.2 7.3 Pinto YM, Elliott PM, Arbustini E, Adler Y, Anastasakis A, Böhm M; et al. (2016). "Proposal for a revised definition of dilated cardiomyopathy, hypokinetic non-dilated cardiomyopathy, and its implications for clinical practice: a position statement of the ESC working group on myocardial and pericardial diseases". Eur Heart J. 37 (23): 1850–8. doi:10.1093/eurheartj/ehv727. PMID 26792875.
- ↑ 8.0 8.1 Bozkurt B, Colvin M, Cook J, Cooper LT, Deswal A, Fonarow GC; et al. (2016). "Current Diagnostic and Treatment Strategies for Specific Dilated Cardiomyopathies: A Scientific Statement From the American Heart Association". Circulation. 134 (23): e579–e646. doi:10.1161/CIR.0000000000000455. PMID 27832612.
- ↑ 9.0 9.1 9.2 Goldberg IJ, Trent CM, Schulze PC (2012). "Lipid metabolism and toxicity in the heart". Cell Metab. 15 (6): 805–12. doi:10.1016/j.cmet.2012.04.006. PMC 3387529. PMID 22682221.
- ↑ 10.0 10.1 Robertson J, Schaufelberger M, Lindgren M, Adiels M, Schiöler L, Torén K; et al. (2019). "Higher Body Mass Index in Adolescence Predicts Cardiomyopathy Risk in Midlife". Circulation. 140 (2): 117–125. doi:10.1161/CIRCULATIONAHA.118.039132. PMC 6635044 Check
|pmc=value (help). PMID 31132859. - ↑ Khan MF, Movahed MR (2013). "Obesity cardiomyopathy and systolic function: obesity is not independently associated with dilated cardiomyopathy". Heart Fail Rev. 18 (2): 207–17. doi:10.1007/s10741-012-9320-4. PMID 22610359.
- ↑ 12.0 12.1 12.2 Madani S, De Girolamo S, Muñoz DM, Li RK, Sweeney G (2006). "Direct effects of leptin on size and extracellular matrix components of human pediatric ventricular myocytes". Cardiovasc Res. 69 (3): 716–25. doi:10.1016/j.cardiores.2005.11.022. PMID 16376323.
- ↑ 13.0 13.1 Abel ED, Litwin SE, Sweeney G (2008). "Cardiac remodeling in obesity". Physiol Rev. 88 (2): 389–419. doi:10.1152/physrev.00017.2007. PMC 2915933. PMID 18391168.
- ↑ Patel DA, Srinivasan SR, Xu JH, Chen W, Berenson GS (2006). "Adiponectin and its correlates of cardiovascular risk in young adults: the Bogalusa Heart Study". Metabolism. 55 (11): 1551–7. doi:10.1016/j.metabol.2006.06.028. PMID 17046560.
- ↑ Merlo M, Zaffalon D, Stolfo D, Altinier A, Barbati G, Zecchin M; et al. (2019). "ECG in dilated cardiomyopathy: specific findings and long-term prognostic significance". J Cardiovasc Med (Hagerstown). 20 (7): 450–458. doi:10.2459/JCM.0000000000000804. PMID 30985353.
- ↑ Momiyama Y, Mitamura H, Kimura M (1994). "ECG characteristics of dilated cardiomyopathy". J Electrocardiol. 27 (4): 323–8. doi:10.1016/s0022-0736(05)80270-5. PMID 7815010.
- ↑ https://litfl.com/wp-content/uploads/2018/08/ECG-Ischaemic-dilated-cardiomyopathy-1.jpg
- ↑ https://litfl.com/wp-content/uploads/2018/08/ECG-Idiopathic-dilated-cardiomyopathy-Biatrial-hypertrophy.jpg
- ↑ Schouten EG, Dekker JM, Meppelink P, Kok FJ, Vandenbroucke JP, Pool J (1991). "QT interval prolongation predicts cardiovascular mortality in an apparently healthy population". Circulation. 84 (4): 1516–23. doi:10.1161/01.cir.84.4.1516. PMID 1914093.
- ↑ Poirier P, Giles TD, Bray GA, Hong Y, Stern JS, Pi-Sunyer FX; et al. (2006). "Obesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight loss: an update of the 1997 American Heart Association Scientific Statement on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism". Circulation. 113 (6): 898–918. doi:10.1161/CIRCULATIONAHA.106.171016. PMID 16380542.
- ↑ Richter C, Richter K, Boewer V (1990). "Significant X-ray patterns in cardiomyopathy--an approach improving noninvasive diagnosis". Cor Vasa. 32 (4): 290–301. PMID 2225878.
- ↑ https://commons.wikimedia.org/wiki/File:DifDilatedCardiomyoMagCXR.png/
- ↑ Thomas DE, Wheeler R, Yousef ZR, Masani ND (2009). "The role of echocardiography in guiding management in dilated cardiomyopathy". Eur J Echocardiogr. 10 (8): iii15–21. doi:10.1093/ejechocard/jep158. PMID 19889654.
- ↑ Mathew T, Williams L, Navaratnam G, Rana B, Wheeler R, Collins K; et al. (2017). "Diagnosis and assessment of dilated cardiomyopathy: a guideline protocol from the British Society of Echocardiography". Echo Res Pract. 4 (2): G1–G13. doi:10.1530/ERP-16-0037. PMC 5574280. PMID 28592613.
- ↑ Lessick J, Mutlak D, Rispler S, Ghersin E, Dragu R, Litmanovich D; et al. (2005). "Comparison of multidetector computed tomography versus echocardiography for assessing regional left ventricular function". Am J Cardiol. 96 (7): 1011–5. doi:10.1016/j.amjcard.2005.05.062. PMID 16188534.
- ↑ Bhatti S, Hakeem A, Yousuf MA, Al-Khalidi HR, Mazur W, Shizukuda Y (2011). "Diagnostic performance of computed tomography angiography for differentiating ischemic vs nonischemic cardiomyopathy". J Nucl Cardiol. 18 (3): 407–20. doi:10.1007/s12350-011-9346-3. PMID 21328027.
- ↑ Levine A, Hecht HS (2015). "Cardiac CT Angiography in Congestive Heart Failure". J Nucl Med. 56 Suppl 4: 46S–51S. doi:10.2967/jnumed.114.150441. PMID 26033904.
- ↑ https://upload.wikimedia.org/wikipedia/commons/3/34/DifCardioMag.png/
- ↑ American College of Cardiology Foundation Task Force on Expert Consensus Documents. Hundley WG, Bluemke DA, Finn JP, Flamm SD, Fogel MA; et al. (2010). "ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents". Circulation. 121 (22): 2462–508. doi:10.1161/CIR.0b013e3181d44a8f. PMC 3034132. PMID 20479157.
{kind=link}
{kind=link}
{kind=link}
{kind=link}