Femoral hernia pathophysiology: Difference between revisions
No edit summary |
|||
| Line 4: | Line 4: | ||
==Overview== | ==Overview== | ||
A femoral hernia is the protrusion of the [[hernia]] sac through the [[femoral ring]] in to the [[femoral canal]]. The [[anatomy]] of the [[femoral canal]] is such that the neck is made up of rigid structures that predispose herniated [[bowel]] to [[strangulation]] and incarceration. The [[hernia]] sac contains [[small bowel]] which can predispose to [[intestinal obstruction]]. Some [[connective tissue diseases]] predispose the patient to developing | A femoral hernia is the protrusion of the [[hernia]] sac through the [[femoral ring]] in to the [[femoral canal]]. The [[anatomy]] of the [[femoral canal]] is such that the neck is made up of rigid structures that predispose herniated [[bowel]] to [[strangulation]] and [[Incarcerated hernia|incarceration]]. The [[hernia]] sac contains [[small bowel]] which can predispose to [[intestinal obstruction]]. Some [[connective tissue diseases]] predispose the patient to developing femoral hernia. [[Malignancy]] is very rarely associated with femoral hernias, thus, [[histopathological]] analysis is done routinely following a repair but shows [[Incarcerated hernia|incarcerated]] [[bowel]] on most occasions. | ||
==Pathophysiology== | ==Pathophysiology== | ||
===Anatomy=== | ===Anatomy=== | ||
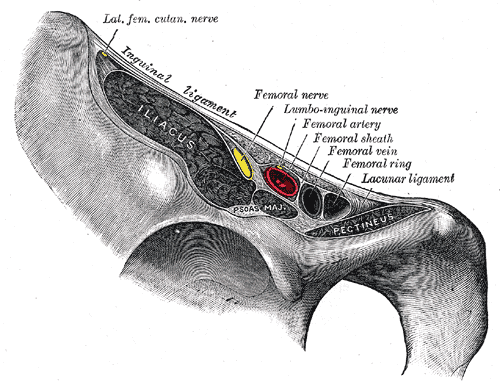
[[File:Gray546.png|300px|thumb|center|'''Contents of the Femoral Canal'''<br>'''Source:''' Henry Vandyke Carter | [[File:Gray546.png|300px|thumb|center|'''Contents of the Femoral Canal'''<br>'''Source:''' Henry Vandyke Carter via Wikimedia Commons<ref name="urlupload.wikimedia.org">{{cite web |url=https://upload.wikimedia.org/wikipedia/commons/7/7d/Gray546.png |title=upload.wikimedia.org |format= |work= |accessdate=}}</ref>]] | ||
*Pelvicrural interval, an opening from the [[abdomen]] to the [[thigh]] is divided in to two spaces:<ref name="pmid17103962">{{cite journal |vauthors=Panton JA |title=Factors bearing upon the Etiology of Femoral Hernia |journal=J. Anat. |volume=57 |issue=Pt 2 |pages=106–46 |year=1923 |pmid=17103962 |pmc=1262989 |doi= |url=}}</ref> | *Pelvicrural interval, an opening from the [[abdomen]] to the [[thigh]], is divided in to two spaces:<ref name="pmid17103962">{{cite journal |vauthors=Panton JA |title=Factors bearing upon the Etiology of Femoral Hernia |journal=J. Anat. |volume=57 |issue=Pt 2 |pages=106–46 |year=1923 |pmid=17103962 |pmc=1262989 |doi= |url=}}</ref> | ||
**Lacuna musculosa ([[lateral]] space), as the name suggests the [[iliopsoas]] muscles pass through this space. | **Lacuna musculosa ([[lateral]] space), as the name suggests the [[iliopsoas]] [[muscles]] pass through this space. | ||
**Lacuna vasculosa (medial space), as the name suggests this is the passage for the [[femoral]] [[vessels]]. | **Lacuna vasculosa ([[medial]] space), as the name suggests this is the passage for the [[femoral]] [[vessels]]. | ||
*In the [[pelvis]] along the [[anterior surface]] of the [[iliopsoas]] [[muscle]] run the [[external iliac]] [[vessels]].<ref name="Lichtenstein">{{cite book | last = Lichtenstein | first = Irving | title = Hernia repair without disability : a surgical atlas illustrating the anatomy, technique, and physiologic rationale of the "one day" hernia and introducing new concepts : tension-free herniorrhapies | publisher = Ishiyaku EuroAmerica | location = St. Louis | year = 1986 | isbn = 0912791306 }}</ref> | *In the [[pelvis]], along the [[anterior surface]] of the [[iliopsoas]] [[muscle]] run the [[external iliac]] [[vessels]].<ref name="Lichtenstein">{{cite book | last = Lichtenstein | first = Irving | title = Hernia repair without disability : a surgical atlas illustrating the anatomy, technique, and physiologic rationale of the "one day" hernia and introducing new concepts : tension-free herniorrhapies | publisher = Ishiyaku EuroAmerica | location = St. Louis | year = 1986 | isbn = 0912791306 }}</ref> | ||
*The [[external iliac]] [[vessels]] pass between the [[iliopubic tract]] and [[Cooper's ligaments|Cooper's ligament]] and then under the [[inguinal ligament]] to become the [[femoral]] [[vessels]].<ref name="Lichtenstein" /> | *The [[external iliac]] [[vessels]] pass between the [[iliopubic tract]] and [[Cooper's ligaments|Cooper's ligament]], and then under the [[inguinal ligament]] to become the [[femoral]] [[vessels]].<ref name="Lichtenstein" /> | ||
*As the [[external iliac]] [[vessels]] pass along the lacuna vasculosa they are covered by the [[transversalis fascia]] forming the [[femoral sheath]].<ref name="Lichtenstein" /> | *As the [[external iliac]] [[vessels]] pass along the lacuna vasculosa, they are covered by the [[transversalis fascia]] forming the [[femoral sheath]].<ref name="Lichtenstein" /> | ||
*The [[femoral sheath]] extends 4cm caudally to become the [[adventitia]] of the [[femoral]] [[vessels]].<ref name="Lichtenstein" /> | *The [[femoral sheath]] extends 4cm [[caudally]] to become the [[adventitia]] of the [[femoral]] [[vessels]].<ref name="Lichtenstein" /> | ||
*The [[femoral sheath]] has a medial compartment that is known as the [[femoral canal]].<ref name="Lichtenstein" /> | *The [[femoral sheath]] has a [[medial]] compartment that is known as the [[femoral canal]].<ref name="Lichtenstein" /> | ||
*The [[femoral canal]] is less than 2 cm in diameter and it contains [[lymphatics]] and [[glands]].<ref name="Lichtenstein" /> | *The [[femoral canal]] is less than 2 cm in diameter and it contains [[lymphatics]] and [[glands]].<ref name="Lichtenstein" /> | ||
*The true opening of the [[femoral canal]] is a musculoaponeurotic ring that consists of:<ref name="pmid4278445">{{cite journal |vauthors=McVay CB |title=The anatomic basis for inguinal and femoral hernioplasty |journal=Surg Gynecol Obstet |volume=139 |issue=6 |pages=931–45 |year=1974 |pmid=4278445 |doi= |url=}}</ref> | *The true opening of the [[femoral canal]] is a musculoaponeurotic ring that consists of:<ref name="pmid4278445">{{cite journal |vauthors=McVay CB |title=The anatomic basis for inguinal and femoral hernioplasty |journal=Surg Gynecol Obstet |volume=139 |issue=6 |pages=931–45 |year=1974 |pmid=4278445 |doi= |url=}}</ref> | ||
**[[Cooper's ligaments|Cooper's ligament]] inferiorly | **[[Cooper's ligaments|Cooper's ligament]] [[inferiorly]] | ||
**[[Femoral vein]] laterally | **[[Femoral vein]] [[Lateral|laterally]] | ||
**[[Iliopubic tract]] superiorly and medially | **[[Iliopubic tract]] [[Superior|superiorly]] and [[medially]] | ||
*The [[medial]] boundary of the [[femoral ring]] is made up of the lateral edge of the [[aponeurosis]] of the insertion of the [[transversus abdominis muscle]] with the [[transversalis fascia]] onto the [[pubis]].<ref name="pmid4278445">{{cite journal |vauthors=McVay CB |title=The anatomic basis for inguinal and femoral hernioplasty |journal=Surg Gynecol Obstet |volume=139 |issue=6 |pages=931–45 |year=1974 |pmid=4278445 |doi= |url=}}</ref> | *The [[medial]] boundary of the [[femoral ring]] is made up of the lateral edge of the [[aponeurosis]] of the insertion of the [[transversus abdominis muscle]] with the [[transversalis fascia]] onto the [[pubis]].<ref name="pmid4278445">{{cite journal |vauthors=McVay CB |title=The anatomic basis for inguinal and femoral hernioplasty |journal=Surg Gynecol Obstet |volume=139 |issue=6 |pages=931–45 |year=1974 |pmid=4278445 |doi= |url=}}</ref> | ||
*The true inner ring of the [[femoral canal]] is bounded:<ref name="pmid14275790">{{cite journal |vauthors=MCVAY CB |title=INGUINAL AND FEMORAL HERNIOPLASTY |journal=Surgery |volume=57 |issue= |pages=615–25 |year=1965 |pmid=14275790 |doi= |url=}}</ref> | *The true inner ring of the [[femoral canal]] is bounded:<ref name="pmid14275790">{{cite journal |vauthors=MCVAY CB |title=INGUINAL AND FEMORAL HERNIOPLASTY |journal=Surgery |volume=57 |issue= |pages=615–25 |year=1965 |pmid=14275790 |doi= |url=}}</ref> | ||
| Line 28: | Line 28: | ||
**Posteriorly by the [[Cooper's ligaments|Cooper's ligament]]. | **Posteriorly by the [[Cooper's ligaments|Cooper's ligament]]. | ||
*The distal [[orifice]] (neck of the [[femoral canal]]) of the [[femoral canal]] has a rigid boundary which is usually less than 1cm in diameter and is surrounded by:<ref name="pmid4280996">{{cite journal |vauthors=Lytle WJ |title=The inguinal and lacunar ligaments |journal=J. Anat. |volume=118 |issue=Pt 2 |pages=241–51 |year=1974 |pmid=4280996 |pmc=1231505 |doi= |url=}}</ref><ref name="pmid18634743">{{cite journal |vauthors=Papanikitas J, Sutcliffe RP, Rohatgi A, Atkinson S |title=Bilateral retrovascular femoral hernia |journal=Ann R Coll Surg Engl |volume=90 |issue=5 |pages=423–4 |year=2008 |pmid=18634743 |pmc=2645754 |doi=10.1308/003588408X301235 |url=}}</ref> | *The distal [[orifice]] (neck of the [[femoral canal]]) of the [[femoral canal]] has a rigid boundary which is usually less than 1cm in diameter and is surrounded by:<ref name="pmid4280996">{{cite journal |vauthors=Lytle WJ |title=The inguinal and lacunar ligaments |journal=J. Anat. |volume=118 |issue=Pt 2 |pages=241–51 |year=1974 |pmid=4280996 |pmc=1231505 |doi= |url=}}</ref><ref name="pmid18634743">{{cite journal |vauthors=Papanikitas J, Sutcliffe RP, Rohatgi A, Atkinson S |title=Bilateral retrovascular femoral hernia |journal=Ann R Coll Surg Engl |volume=90 |issue=5 |pages=423–4 |year=2008 |pmid=18634743 |pmc=2645754 |doi=10.1308/003588408X301235 |url=}}</ref> | ||
**The [[lacunar ligament]] medially | **The [[lacunar ligament]] [[medially]] | ||
**The [[inguinal ligament]] anteriorly | **The [[inguinal ligament]] [[Anterior|anteriorly]] | ||
**[[Fascia]] of the pectineal muscle posteriorly | **[[Fascia]] of the [[Pectineus muscle|pectineal muscle]] [[Posterior|posteriorly]] | ||
**The rigidity of these structures is the reason for [[strangulation]] in [[Femoral hernia|femoral hernias]]. | **The rigidity of these structures is the reason for [[strangulation]] in [[Femoral hernia|femoral hernias]]. | ||
===Pathogenesis=== | ===Pathogenesis=== | ||
*A [[femoral hernia]] is the protrusion of the [[peritoneal]] sac through the [[femoral ring]] in to the [[femoral canal]] [[posterior]] and inferior to the [[inguinal ligament]] and it is [[medial]] to the [[femoral]] [[vessels]].<ref name="Doherty">{{cite book | last = Doherty | first = Gerard | title = Current diagnosis & treatment : surgery | publisher = Lange Medical Books/McGraw-Hill | location = New York | year = 2010 | isbn = 978-0071635158 }}</ref> | *A [[femoral hernia]] is the protrusion of the [[peritoneal]] sac through the [[femoral ring]] in to the [[femoral canal]], [[posterior]] and inferior to the [[inguinal ligament]], and it is [[medial]] to the [[femoral]] [[vessels]].<ref name="Doherty">{{cite book | last = Doherty | first = Gerard | title = Current diagnosis & treatment : surgery | publisher = Lange Medical Books/McGraw-Hill | location = New York | year = 2010 | isbn = 978-0071635158 }}</ref> | ||
*The [[hernia]] sac | *The [[hernia]] sac may contain preperitoneal [[fat]], [[omentum]] or [[small bowel]].<ref name="Doherty" /> | ||
*Femoral hernias typically have a narrow [[neck]], which predisposes them to incarceration and the need for emergent surgery.<ref name="Doherty" /> | *Femoral hernias typically have a narrow [[neck]], which predisposes them to incarceration and the need for emergent surgery.<ref name="Doherty" /> | ||
*De Garengeot [[hernia]] is a type of femoral hernia that contains the [[appendix]].<ref name="pmid21442431">{{cite journal |vauthors=Phillips AW, Aspinall SR |title=Appendicitis and Meckel's diverticulum in a femoral hernia: simultaneous De Garengeot and Littre's hernia |journal=Hernia |volume=16 |issue=6 |pages=727–9 |year=2012 |pmid=21442431 |doi=10.1007/s10029-011-0812-2 |url=}}</ref> | *De Garengeot [[hernia]] is a type of femoral hernia that contains the [[appendix]].<ref name="pmid21442431">{{cite journal |vauthors=Phillips AW, Aspinall SR |title=Appendicitis and Meckel's diverticulum in a femoral hernia: simultaneous De Garengeot and Littre's hernia |journal=Hernia |volume=16 |issue=6 |pages=727–9 |year=2012 |pmid=21442431 |doi=10.1007/s10029-011-0812-2 |url=}}</ref> | ||
| Line 41: | Line 41: | ||
==Genetics== | ==Genetics== | ||
*First degree relatives of patients with [[inguinal hernia]] are more susceptible to developing femoral hernia.<ref name="pmid9225924">{{cite journal |vauthors=Liem MS, van der Graaf Y, Beemer FA, van Vroonhoven TJ |title=Increased risk for inguinal hernia in patients with Ehlers-Danlos syndrome |journal=Surgery |volume=122 |issue=1 |pages=114–5 |year=1997 |pmid=9225924 |doi= |url=}}</ref><ref name="pmid26686553">{{cite journal |vauthors=Jorgenson E, Makki N, Shen L, Chen DC, Tian C, Eckalbar WL, Hinds D, Ahituv N, Avins A |title=A genome-wide association study identifies four novel susceptibility loci underlying inguinal hernia |journal=Nat Commun |volume=6 |issue= |pages=10130 |year=2015 |pmid=26686553 |pmc=4703831 |doi=10.1038/ncomms10130 |url=}}</ref> | *[[First degree relative|First degree relatives]] of patients with [[inguinal hernia]] are more susceptible to developing femoral hernia.<ref name="pmid9225924">{{cite journal |vauthors=Liem MS, van der Graaf Y, Beemer FA, van Vroonhoven TJ |title=Increased risk for inguinal hernia in patients with Ehlers-Danlos syndrome |journal=Surgery |volume=122 |issue=1 |pages=114–5 |year=1997 |pmid=9225924 |doi= |url=}}</ref><ref name="pmid26686553">{{cite journal |vauthors=Jorgenson E, Makki N, Shen L, Chen DC, Tian C, Eckalbar WL, Hinds D, Ahituv N, Avins A |title=A genome-wide association study identifies four novel susceptibility loci underlying inguinal hernia |journal=Nat Commun |volume=6 |issue= |pages=10130 |year=2015 |pmid=26686553 |pmc=4703831 |doi=10.1038/ncomms10130 |url=}}</ref> | ||
==Associated Conditions== | ==Associated Conditions== | ||
| Line 55: | Line 55: | ||
==Microscopic Pathology== | ==Microscopic Pathology== | ||
*It is recommended that femoral hernia specimens should be submitted for microscopic histopathological analysis, though it is very rare to find a [[malignant]] lesion in a femoral hernia sac.<ref name="pmid23794497">{{cite journal |vauthors=Wang T, Vajpeyi R |title=Hernia sacs: is histological examination necessary? |journal=J. Clin. Pathol. |volume=66 |issue=12 |pages=1084–6 |year=2013 |pmid=23794497 |doi=10.1136/jclinpath-2013-201734 |url=}}</ref> | *It is recommended that femoral hernia specimens should be submitted for [[microscopic]] [[histopathological]] analysis, though it is very rare to find a [[malignant]] lesion in a femoral hernia sac.<ref name="pmid23794497">{{cite journal |vauthors=Wang T, Vajpeyi R |title=Hernia sacs: is histological examination necessary? |journal=J. Clin. Pathol. |volume=66 |issue=12 |pages=1084–6 |year=2013 |pmid=23794497 |doi=10.1136/jclinpath-2013-201734 |url=}}</ref> | ||
==References== | ==References== | ||
Revision as of 15:45, 15 February 2018
|
Femoral hernia Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Femoral hernia pathophysiology On the Web |
|
American Roentgen Ray Society Images of Femoral hernia pathophysiology |
|
Risk calculators and risk factors for Femoral hernia pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: M. Khurram Afzal, MD [2]
Overview
A femoral hernia is the protrusion of the hernia sac through the femoral ring in to the femoral canal. The anatomy of the femoral canal is such that the neck is made up of rigid structures that predispose herniated bowel to strangulation and incarceration. The hernia sac contains small bowel which can predispose to intestinal obstruction. Some connective tissue diseases predispose the patient to developing femoral hernia. Malignancy is very rarely associated with femoral hernias, thus, histopathological analysis is done routinely following a repair but shows incarcerated bowel on most occasions.
Pathophysiology
Anatomy

Source: Henry Vandyke Carter via Wikimedia Commons[1]
- Pelvicrural interval, an opening from the abdomen to the thigh, is divided in to two spaces:[2]
- In the pelvis, along the anterior surface of the iliopsoas muscle run the external iliac vessels.[3]
- The external iliac vessels pass between the iliopubic tract and Cooper's ligament, and then under the inguinal ligament to become the femoral vessels.[3]
- As the external iliac vessels pass along the lacuna vasculosa, they are covered by the transversalis fascia forming the femoral sheath.[3]
- The femoral sheath extends 4cm caudally to become the adventitia of the femoral vessels.[3]
- The femoral sheath has a medial compartment that is known as the femoral canal.[3]
- The femoral canal is less than 2 cm in diameter and it contains lymphatics and glands.[3]
- The true opening of the femoral canal is a musculoaponeurotic ring that consists of:[4]
- The medial boundary of the femoral ring is made up of the lateral edge of the aponeurosis of the insertion of the transversus abdominis muscle with the transversalis fascia onto the pubis.[4]
- The true inner ring of the femoral canal is bounded:[5]
- Anteriorly and medially by the iliopubic tract.
- Posteriorly by the Cooper's ligament.
- The distal orifice (neck of the femoral canal) of the femoral canal has a rigid boundary which is usually less than 1cm in diameter and is surrounded by:[6][7]
- The lacunar ligament medially
- The inguinal ligament anteriorly
- Fascia of the pectineal muscle posteriorly
- The rigidity of these structures is the reason for strangulation in femoral hernias.
Pathogenesis
- A femoral hernia is the protrusion of the peritoneal sac through the femoral ring in to the femoral canal, posterior and inferior to the inguinal ligament, and it is medial to the femoral vessels.[8]
- The hernia sac may contain preperitoneal fat, omentum or small bowel.[8]
- Femoral hernias typically have a narrow neck, which predisposes them to incarceration and the need for emergent surgery.[8]
- De Garengeot hernia is a type of femoral hernia that contains the appendix.[9]
- Littre hernia is an uncommon type of femoral hernia that contains a Meckel's diverticulum.[9]
Genetics
- First degree relatives of patients with inguinal hernia are more susceptible to developing femoral hernia.[10][11]
Associated Conditions
- Ehlers-Danlos syndrome[10][12][13]
- Appendicitis[9][14][15][16]
- Meckel's diverticulum[17][9][18]
- Intestinal obstruction[18]
- Intestinal volvulus[18]
- Intussusception[18]
Gross Pathology
Microscopic Pathology
- It is recommended that femoral hernia specimens should be submitted for microscopic histopathological analysis, though it is very rare to find a malignant lesion in a femoral hernia sac.[19]
References
- ↑ "upload.wikimedia.org".
- ↑ Panton JA (1923). "Factors bearing upon the Etiology of Femoral Hernia". J. Anat. 57 (Pt 2): 106–46. PMC 1262989. PMID 17103962.
- ↑ 3.0 3.1 3.2 3.3 3.4 3.5 Lichtenstein, Irving (1986). Hernia repair without disability : a surgical atlas illustrating the anatomy, technique, and physiologic rationale of the "one day" hernia and introducing new concepts : tension-free herniorrhapies. St. Louis: Ishiyaku EuroAmerica. ISBN 0912791306.
- ↑ 4.0 4.1 McVay CB (1974). "The anatomic basis for inguinal and femoral hernioplasty". Surg Gynecol Obstet. 139 (6): 931–45. PMID 4278445.
- ↑ MCVAY CB (1965). "INGUINAL AND FEMORAL HERNIOPLASTY". Surgery. 57: 615–25. PMID 14275790.
- ↑ Lytle WJ (1974). "The inguinal and lacunar ligaments". J. Anat. 118 (Pt 2): 241–51. PMC 1231505. PMID 4280996.
- ↑ Papanikitas J, Sutcliffe RP, Rohatgi A, Atkinson S (2008). "Bilateral retrovascular femoral hernia". Ann R Coll Surg Engl. 90 (5): 423–4. doi:10.1308/003588408X301235. PMC 2645754. PMID 18634743.
- ↑ 8.0 8.1 8.2 Doherty, Gerard (2010). Current diagnosis & treatment : surgery. New York: Lange Medical Books/McGraw-Hill. ISBN 978-0071635158.
- ↑ 9.0 9.1 9.2 9.3 Phillips AW, Aspinall SR (2012). "Appendicitis and Meckel's diverticulum in a femoral hernia: simultaneous De Garengeot and Littre's hernia". Hernia. 16 (6): 727–9. doi:10.1007/s10029-011-0812-2. PMID 21442431.
- ↑ 10.0 10.1 Liem MS, van der Graaf Y, Beemer FA, van Vroonhoven TJ (1997). "Increased risk for inguinal hernia in patients with Ehlers-Danlos syndrome". Surgery. 122 (1): 114–5. PMID 9225924.
- ↑ Jorgenson E, Makki N, Shen L, Chen DC, Tian C, Eckalbar WL, Hinds D, Ahituv N, Avins A (2015). "A genome-wide association study identifies four novel susceptibility loci underlying inguinal hernia". Nat Commun. 6: 10130. doi:10.1038/ncomms10130. PMC 4703831. PMID 26686553.
- ↑ Harrison B, Sanniec K, Janis JE (2016). "Collagenopathies-Implications for Abdominal Wall Reconstruction: A Systematic Review". Plast Reconstr Surg Glob Open. 4 (10): e1036. doi:10.1097/GOX.0000000000001036. PMC 5096520. PMID 27826465.
- ↑ Lei W, Huang J, Luoshang C (2012). "New minimally invasive technique for repairing femoral hernias: 3-D patch device through a femoris approach". Can J Surg. 55 (3): 177–80. doi:10.1503/cjs.030710. PMC 3364305. PMID 22630060.
- ↑ Kalles V, Mekras A, Mekras D, Papapanagiotou I, Al-Harethee W, Sotiropoulos G, Liakou P, Kastania A, Piperos T, Mariolis-Sapsakos T (2013). "De Garengeot's hernia: a comprehensive review". Hernia. 17 (2): 177–82. doi:10.1007/s10029-012-0993-3. PMID 22983696.
- ↑ Snoekx R, Geyskens P (2014). "De Garengeot's hernia: acute appendicitis in a femoral hernia. Case report and literature overview". Acta Chir. Belg. 114 (2): 149–51. PMID 25073217.
- ↑ Sinraj AP, Anekal N, Rathnakar SK (2016). "De Garengeot's Hernia - A Diagnostic and Therapeutic Challenge". J Clin Diagn Res. 10 (11): PD19–PD20. doi:10.7860/JCDR/2016/21522.8871. PMC 5198391. PMID 28050438.
- ↑ Zacharakis E, Papadopoulos V, Athanasiou T, Ziprin P, Zacharakis E (2008). "An unusual presentation of Meckel diverticulum as strangulated femoral hernia". South. Med. J. 101 (1): 96–8. doi:10.1097/SMJ.0b013e31815d3c83. PMID 18176301.
- ↑ 18.0 18.1 18.2 18.3 Wu SY, Ho MH, Hsu SD (2014). "Meckel's diverticulum incarcerated in a transmesocolic internal hernia". World J. Gastroenterol. 20 (37): 13615–9. doi:10.3748/wjg.v20.i37.13615. PMC 4188914. PMID 25309093.
- ↑ 19.0 19.1 Wang T, Vajpeyi R (2013). "Hernia sacs: is histological examination necessary?". J. Clin. Pathol. 66 (12): 1084–6. doi:10.1136/jclinpath-2013-201734. PMID 23794497.
{kind=link}