Chronic bronchitis epidemiology and demographics
|
Chronic bronchitis Microchapters |
|
Diagnosis |
|
Treatment |
|
Case Studies |
|
Chronic bronchitis epidemiology and demographics On the Web |
|
American Roentgen Ray Society Images of Chronic bronchitis epidemiology and demographics |
|
Chronic bronchitis epidemiology and demographics in the news |
|
Risk calculators and risk factors for Chronic bronchitis epidemiology and demographics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief:
Overview
COPD occurs in 34 out of 1000 greater than 65 years old. In England, an estimated 842,100 of 50 million people have a diagnosis of COPD; translating into approximately one person in 59 receiving a diagnosis of COPD at some point in their lives. In the most socioeconomically deprived parts of the country, one in 32 people were diagnosed with COPD, compared with one in 98 in the most affluent areas. In the United States, the prevalence of COPD is approximately 1 in 20 or 5%, totalling approximately 13.5 million people in USA,[1] or possibly approximately 25 million people if undiagnosed cases are included.[2]
Epidemiology and Demographics
Epidemiology and Demographics
Developed Countries
USA
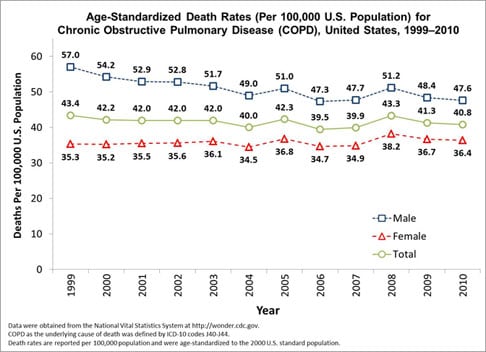
Mortality
- During 2000--2005, COPD was the underlying cause of death for 718,077 persons overall aged >25 years in the United States. The number of deaths from COPD increased from 116,494 in 2000 to 121,267 in 2003, decreased to 117,134 in 2004, and increased to 126,005 in 2005.
- To update national estimates of deaths from COPD for the period 2000-2005 (the most recent years for which data are available), CDC analyzed data from the National Vital Statistics System (NVSS). Results of that analysis indicated that an estimated 126,005 deaths of persons aged >25 years occurred in 2005 with COPD as the underlying cause, an increase of 8% from 116,494 deaths in 2000.
- In 2005, approximately one in 20 deaths in the United States had COPD as the underlying cause.
- Smoking is estimated to be responsible for at least 75% of COPD deaths.
Age
- Age-standardized COPD mortality rates remained fairly stable during the period (2000-2005) overall. Age-standardized death rates per 100,000 population decreased during 2000--2004; the rate in 2005 was similar to that for 2003.
Race
- For each year during 2000--2005, COPD mortality rates were higher among whites than among blacks or persons of all other races. During this period, the rate for blacks remained stable, except for 2004, when the rate was lower. In 2005, the death rate among white men was 80.2 (95% confidence interval [CI] = 79.5--80.9) compared with 63.8 (CI = 61.8--65.8) among black men, 60.3 (CI = 59.8--60.8) among white women, and 29.9 (CI = 28.9--30.9) among black women.
Gender
- From 2000 to 2005, the annual number of deaths from COPD increased 5% among men, and the number of deaths was higher in 2005 than in 2004. The death rate for men declined during 2000--2005 and was lower in 2004 than in 2005. Among women, the annual number of deaths increased 11% from 2000 to 2005 and was lower in 2005 than in 2004. The death rate for women increased from 2000 to 2003, decreased in 2004, and increased in 2005. The death rate was higher for men compared with the rate for women in each year, but the number of deaths was greater for women. For women, the number of deaths related to COPD in 2005 was 65,193, while for men it was 60,812.
Economical Impact
- The total economic costs of COPD in the United States were estimated to be $49.9 billion in 2010, and the total direct cost of medical care is approximately $29.5 billion per year.[3] Excess health-care expenditures are estimated at nearly $6,000 annually for every COPD patient in the United States.
States Based Statistics
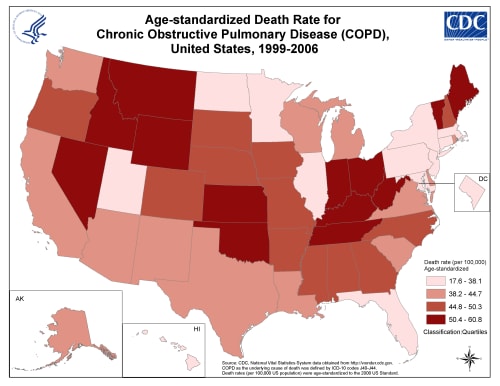
- By state, in 2005, age-standardized death rates from COPD for adults aged >25 years ranged from 27.1 per 100,000 in Hawaii to 93.6 per 100,000 population in Oklahoma. States with COPD death rates in the highest quartile were as follows: Idaho, Indiana, Kansas, Kentucky, Maine, Montana, Nevada, Ohio, Oklahoma, Vermont, West Virginia, and Wyoming. Among adults aged 25--64 years, rates ranged from 6.2 (Massachusetts and New Jersey) to 19.2 (Oklahoma) per 100,000 population for men and from 3.8 (New Jersey) to 16.5 (West Virginia) in women. Among adults aged >65 years, rates ranged from 169.0 (Hawaii) to 540.4 (Vermont) per 100,000 population in men and from 94.7 (Hawaii) to 394.9 (Nevada) in women.
Statistics
Work Related Lung Disease (World) Surveillance System
This CDC national surveillance system is maintained by the National Institute for Occupational Safety and Health (NIOSH) and includes up-to-date summary tables, graphs, and figures of occupationally-related respiratory disease surveillance data on the pneumoconioses, occupational asthma and other airways diseases, and several other respiratory conditions including chronic obstructive pulmonary disease. Information is available at http://www2a.cdc.gov/drds/WorldReportData/.
http://www.cdc.gov/copd/images/copd_graph.jpg
{kind=link}
Prevalence in the United States
http://www.cdc.gov/copd/images/copd_map.png
{kind=link}
Age-standardized death rates for chronic obstructive pulmonary disease (COPD), by state, aggregated over 1999–2006. State rates are grouped into quartiles. Data were obtained from the National Vital Statistics System at http://wonder.cdc.gov. COPD as the underlying cause of death was defined by ICD-10 codes J40-J44. Death rates are reported per 100,000 population and were age-standardized to the 2000 U.S. standard population
External Links
http://www.cdc.gov/copd/data.htm
References
- ↑ wrongdiagnosis.com > Prevalence and Incidence of COPD Retrieved on Mars 14, 2010
- ↑ MORBIDITY & MORTALITY: 2009 CHART BOOK ON CARDIOVASCULAR, LUNG, AND BLOOD DISEASES National Heart, Lung, and Blood Institute
- ↑ [A Q, J WT, E WS, et al. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Annals of internal medicine 2011;155:179-91]