Coronary angiography standard views
|
Coronary Angiography | |
|
General Principles | |
|---|---|
|
Anatomy & Projection Angles | |
|
Normal Anatomy | |
|
Anatomic Variants | |
|
Projection Angles | |
|
Epicardial Flow & Myocardial Perfusion | |
|
Epicardial Flow | |
|
Myocardial Perfusion | |
|
Lesion Complexity | |
|
ACC/AHA Lesion-Specific Classification of the Primary Target Stenosis | |
|
Lesion Morphology | |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
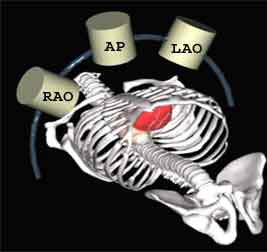
Standard Angiographic Views
Rotation describes the position of the image intensifier around the longitudinal axis of the patient. LAO refers to rotating the camera to the patient's left (catheter and spine will be on the right side of the image), RAO to the patient's right (catheter and spine on the left side of the image). Angulation describes the position of the image intensifier in the short axis of the patient. Camera can pivit toward (cranial) or away (caudal) from the patient's head. Diagram
{kind=link}
For the beginner angiographer the anatomic landmarks formed by the spine, catheter and diaphragm provide information to discern which tomographic view from which the image is obtained. In the LAO view (figure 1) the catheter and spine are seen on the right side of the image, while in the RAO (figure 2) they are found on the left. PA imaging (figure 3) places these landmarks in the center of the image. Cranial angulation can usually be distinguished from caudal angulation by the presence of the diaphragm. For cranial imaging, the patient should be asked to inspire to remove the diaphragmatic shadow from the image.
Post-surgical Views
- Left Lateral; LIMA (body)
- Right Cranial; LIMA to mid LAD
- Right Caudal; LIMA to distal LAD
- Left Lateral; LIMA to distal LAD
- Right Cranial; LIMA to diagonal arteries
- Left Lateral SVG to LAD
 |
 |
 |
Left Coronary Artery
The left main coronary artery gives rise to the left anterior descending artery and the left circumflex coronary artery. Complete visualization of these arteries and their branches requires care and rigor to ensure complete anatomical documentation. Often bifurcations and vessel foreshortening and overlap cause errors in stenosis estimation. There are no steadfast rules in which tomographic views are most useful. Generally, for circumflex and proximal epicardial visualization the caudal views are most useful. For LAD and LAD/diagonal bifurcation visualization the cranial views are most useful. Overall, if there is not a significant limitation on contrast utilization, standard 'around the world' angiography using a selection of the following angiographic views will document left coronary anatomy.
RAO 20 - Caudal 20
 |
RAO Cranial
{{#ev:youtube|5oFB_PZMquc}}
AP 0 - Caudal 30
 |
LAO 50 - Caudal 30
 |
LAO 50 - Cranial 30
 |
AP 0 - Cranial 40
 |
Right Coronary Artery
LAO View
Initial angiographic imaging of the RCA in this view (LAO 30) gives the best view of significant ostial and proximal RCA disease.
{{#ev:youtube|ZtMKl27S-DE}}
RAO View
The mid RCA is best visualized in the straight RAO 30 position.
{{#ev:youtube|8Q83-f-mgY4}}
AP 0 Cranial 30 View
The bifurcation of the distal RCA and rPDA is best seen in the AP 0 Cranial 30 view with a small breath in.
{{#ev:youtube|zTwLSi0-b94}}