Temporal arteritis pathophysiology
|
Temporal Arteritis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Temporal arteritis pathophysiology On the Web |
|
American Roentgen Ray Society Images of Temporal arteritis pathophysiology |
|
Risk calculators and risk factors for Temporal arteritis pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hamid Qazi, MD, BSc [2]
Overview
Temporal arteritis is caused by transmural inflammation of elastic arteries. It is understood that temporal arteritis is the result of cell mediated immunity which arises as a response to endothelial injury and is antigen-driven disease with T-cell and macrophage activation in the elastic tissue in the arterial walls. The adventitia of the vessel is the initial site of immunologic injury. The activation of dendritic cells in the adventitia causes a production of chemokines that recruit CD4+ T helper cells. The CD4+ T helper cell convert in to Th17 cells which produce interleukin 17 and Th1 cells which produce interferon gamma. Giant cell are one of many inflammatory cells that are recruited and produce growth factor which narrows and obstructs the vessels. The concentric inflammation occurs in segments. Macrophages in the adventitia produce interleukin 6. While in the intima and media of the vessel, macrophages produce vascular endothelial growth factor (VEGF) and metalloproteinases which destroy the internal elastic lamina. An increased activated platelets express P-selectin which may cause vessel inflammation and thromboembolic events. Temporal arteritis arises from giant cells, which are fused monocytes cells that are normally involved in the body immune response. Because the disease involves only arteries with internal elastic lamina, the aortic arch and its branches are often involved. Intracranial arteries do not have internal elastic lamina and are not involved.
Pathophysiology
Pathogenesis
- Temporal arteritis is the result of cell mediated immunity which arises as a response to endothelial injury and is an antigen-driven disease with local T-cell and macrophage activation in the elastic tissue of arterial walls with an important role of the proinflammatory cytokines.[1][2][3][4]
- The adventitia of the vessel is the initial site of immunologic injury. The activation of dendritic cells in the adventitia causes a production of chemokines that recruit CD4+ T helper cells. The CD4+ T helper cell convert in to Th17 cells which produce interleukin 17 and Th1 cells which produce interferon gamma.
- Giant cell are one of many inflammatory cells that are recruited and produce growth factor which narrows and obstructs the vessels.[5][6]
- The concentric inflammation occurs in segments.[7]
- Macrophages in the adventitia produce interleukin 6. While in the intima and media of the vessel, macrophages produce vascular endothelial growth factor (VEGF) and metalloproteinases which destroy the internal elastic lamina.[6]
- An increased activated platelets express P-selectin which may cause vessel inflammation and thromboembolic events.[8]
- Temporal arteritis arises from giant cells, which are fused monocytes cells that are normally involved in the body immune response.
- Because the disease involves only arteries with internal elastic lamina, the aortic arch and its branches are often involved. Intracranial arteries do not have internal elastic lamina and are not involved.
Commonly involved sites:[9][10][11][12]
- Cervicocephalic arteries: Carotid artery and vertebral artery. The vertebral artery is involved as frequently as the temporal artery in fatal cases. Involvement of the basilar artery is rare.
- Intraorbital branches: Posterior ciliary artery and ophthalmic artery.
- External common, external, and internal carotid artery involvement: It is less common for proximal intracranial arteries to be involved.
- External vertebral arteries: It is less common though for the disease to extend more than 5 mm beyond the dural penetration.
- Subclavian, axially and proximal brachial artery: There can be typical vasculitic lesions with long, smooth, lesions with tapered occlusions.
- Coronary arteries: For a full discussion of the involvement of the heart in this disorder see the chapter on The Heart in Temporal Arteritis / Giant Cell Arteritis
Less commonly involved sites:[11]
- Descending aorta: Mesenteric, iliac, femoral and renal arteries are less often involved. In these cases mesenteric ischemia, renal infarction, and ischemic mononeuropathy can occur.
Genetics
- Temporal artertis has an association with the HLA-DR4 haplotype.[13]
- An association between Toll-like receptor 4 gene polymorphism temporal arteritis has been found.[14]
Associated Conditions
- Temporal arteritis may coexist (in one quarter of cases) with polymyalgia rheumatica (PMR), which is characterized by a sudden onset of pain and stiffness in muscles (pelvis, shoulder) of the body and seen in the elderly.[15][16] Other diseases related with temporal arteritis are systemic lupus erythematosus, rheumatoid arthritis and severe infections.[17][18][19]
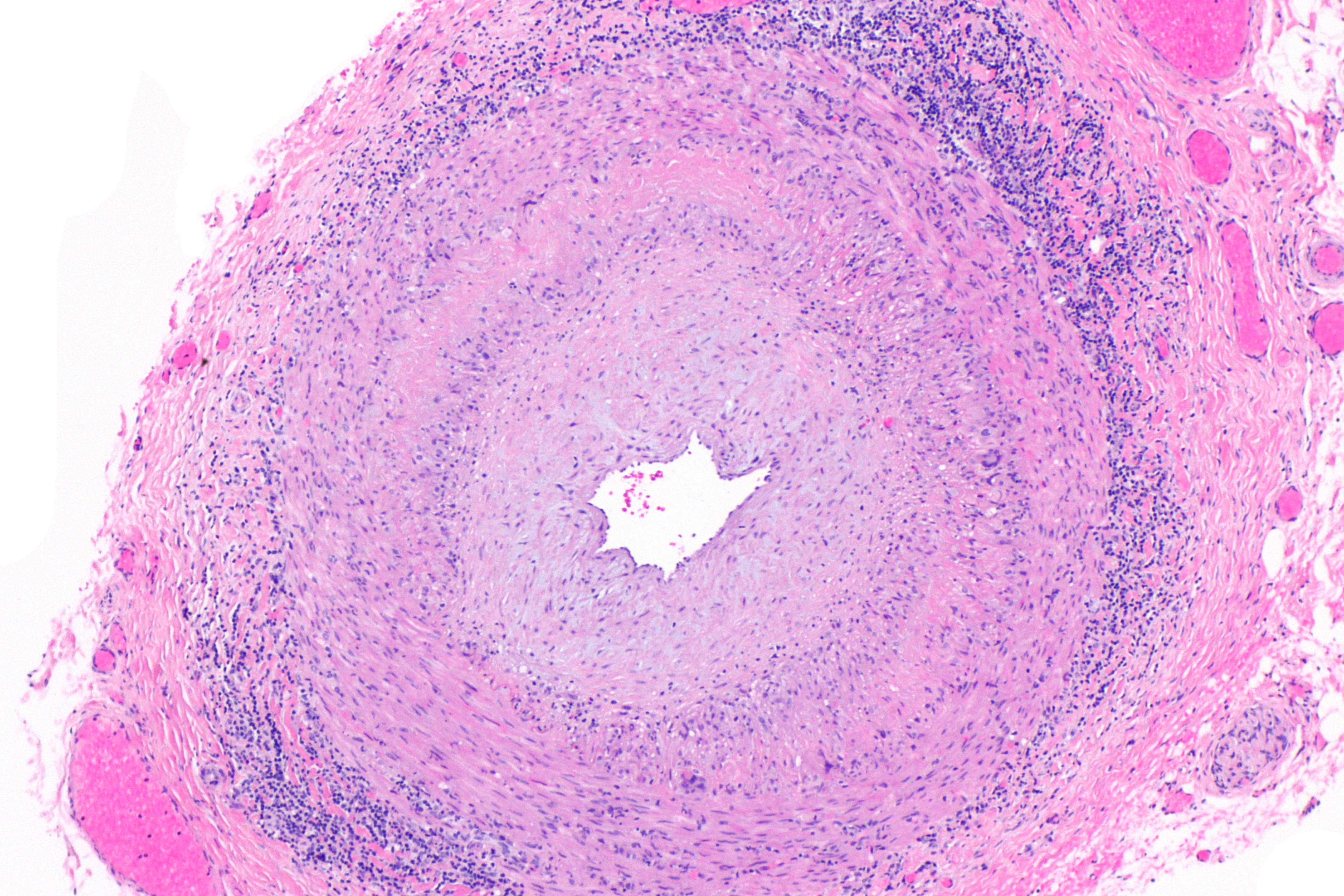
Microscopic Pathology
- On microscopic histopathological analysis the characteristic findings of temporal arteritis are:[20][21][4]
- Skip lesions and normal intervening segments
- Intimal thickening, with prominent cellular infiltration
- Lymphocytes in the internal or external elastic lamina or adventitia
- Areas of necrosis may be present in the arterial wall
- Granulomas containing multinucleated histiocytic and foreign body giant cells, helper T-cell lymphocytes, plasma cells, and fibroblasts[22]

{kind=link}
Video
{{#ev:youtube|UrGsVfLbnA0}}
{{#ev:youtube|wBh4bI7Do3s}}
References
- ↑ Salvarani, C.; Pipitone, N.; Boiardi, L.; Hunder, G. G (2007). "Do we need treatment with tumour necrosis factor blockers for giant cell arteritis?". Annals of the Rheumatic Diseases. 67 (5): 577–579. doi:10.1136/ard.2007.086330. ISSN 0003-4967.
- ↑ Pache M, Kaiser HJ, Haufschild T, Lübeck P, Flammer J (2002). "Increased endothelin-1 plasma levels in giant cell arteritis: a report on four patients". Am J Ophthalmol. 133 (1): 160–2. PMID 11755863.
- ↑ Patel SJ, Lundy DC (2002). "Ocular manifestations of autoimmune disease". Am Fam Physician. 66 (6): 991–8. PMID 12358224.
- ↑ 4.0 4.1 Wang AL, Raven ML, Surapaneni K, Albert DM (2017). "Studies on the Histopathology of Temporal Arteritis". Ocul Oncol Pathol. 3 (1): 60–65. doi:10.1159/000449466. PMC 5318845. PMID 28275606.
- ↑ Samson, Maxime; Corbera-Bellalta, Marc; Audia, Sylvain; Planas-Rigol, Ester; Martin, Laurent; Cid, Maria Cinta; Bonnotte, Bernard (2017). "Recent advances in our understanding of giant cell arteritis pathogenesis". Autoimmunity Reviews. 16 (8): 833–844. doi:10.1016/j.autrev.2017.05.014. ISSN 1568-9972.
- ↑ 6.0 6.1 Eberhardt RT, Dhadly M (2007). "Giant cell arteritis: diagnosis, management, and cardiovascular implications". Cardiol Rev. 15 (2): 55–61. doi:10.1097/01.crd.0000218853.05856.b6. PMID 17303991.
- ↑ Diaz, Vicente A.; DeBroff, Brian M.; Sinard, John (2005). "Comparison of Histopathologic Features, Clinical Symptoms, and Erythrocyte Sedimentation Rates in Biopsy-Positive Temporal Arteritis". Ophthalmology. 112 (7): 1293–1298. doi:10.1016/j.ophtha.2005.02.016. ISSN 0161-6420.
- ↑ Goodwin JS (1992). "Progress in gerontology: polymyalgia rheumatica and temporal arteritis". J Am Geriatr Soc. 40 (5): 515–25. PMID 1634709.
- ↑ Waldman, Corey W.; Waldman, Steven D.; Waldman, Reid A. (2013). "Giant Cell Arteritis". Medical Clinics of North America. 97 (2): 329–335. doi:10.1016/j.mcna.2012.12.006. ISSN 0025-7125.
- ↑ Pineles, Stacy L.; Arnold, Anthony C. (2007). "Giant Cell Arteritis". International Ophthalmology Clinics. 47 (4): 105–119. doi:10.1097/IIO.0b013e318157fb08. ISSN 0020-8167.
- ↑ 11.0 11.1 Liozon, E.; Ly, K.-H.; Robert, P.-Y. (2013). "Manifestations ophtalmologiques de la maladie de Horton". La Revue de Médecine Interne. 34 (7): 421–430. doi:10.1016/j.revmed.2013.02.030. ISSN 0248-8663.
- ↑ Wilkinson IM, Russell RW (1972). "Arteries of the head and neck in giant cell arteritis. A pathological study to show the pattern of arterial involvement". Arch Neurol. 27 (5): 378–91. PMID 5078894.
- ↑ Liozon E, Ouattara B, Rhaiem K, Ly K, Bezanahary H, Loustaud V; et al. (2009). "Familial aggregation in giant cell arteritis and polymyalgia rheumatica: a comprehensive literature review including 4 new families". Clin Exp Rheumatol. 27 (1 Suppl 52): S89–94. PMID 19646354.
- ↑ Palomino-Morales R, Torres O, Vazquez-Rodriguez TR, Morado IC, Castañeda S, Callejas-Rubio JL; et al. (2009). "Association between toll-like receptor 4 gene polymorphism and biopsy-proven giant cell arteritis". J Rheumatol. 36 (7): 1501–6. doi:10.3899/jrheum.081286. PMID 19531762.
- ↑ Caylor TL, Perkins A (2013). "Recognition and management of polymyalgia rheumatica and giant cell arteritis". Am Fam Physician. 88 (10): 676–84. PMID 24364483.
- ↑ Salvarani, Carlo; Cantini, Fabrizio; Hunder, Gene G (2008). "Polymyalgia rheumatica and giant-cell arteritis". The Lancet. 372 (9634): 234–245. doi:10.1016/S0140-6736(08)61077-6. ISSN 0140-6736.
- ↑ Alvarez-Lafuente, R (2005). "Human parvovirus B19, varicella zoster virus, and human herpes virus 6 in temporal artery biopsy specimens of patients with giant cell arteritis: analysis with quantitative real time polymerase chain reaction". Annals of the Rheumatic Diseases. 64 (5): 780–782. doi:10.1136/ard.2004.025320. ISSN 0003-4967.
- ↑ Russo MG, Waxman J, Abdoh AA, Serebro LH (1995). "Correlation between infection and the onset of the giant cell (temporal) arteritis syndrome. A trigger mechanism?". Arthritis Rheum. 38 (3): 374–80. PMID 7880192.
- ↑ Gilden, Don; Nagel, Maria (2015). "Varicella Zoster Virus in Temporal Arteries of Patients With Giant Cell Arteritis". Journal of Infectious Diseases. 212 (suppl 1): S37–S39. doi:10.1093/infdis/jiu542. ISSN 0022-1899.
- ↑ Pountain G, Hazleman B (1995). "ABC of rheumatology. Polymyalgia rheumatica and giant cell arteritis". BMJ. 310 (6986): 1057–9. PMC 2549437. PMID 7728064.
- ↑ Weyand CM, Fulbright JW, Hunder GG, Evans JM, Goronzy JJ (2000). "Treatment of giant cell arteritis: interleukin-6 as a biologic marker of disease activity". Arthritis Rheum. 43 (5): 1041–8. doi:10.1002/1529-0131(200005)43:5<1041::AID-ANR12>3.0.CO;2-7. PMID 10817557.
- ↑ Liozon E, Ly KH, Robert PY (2013). "[Ocular complications of giant cell arteritis]". Rev Med Interne. 34 (7): 421–30. doi:10.1016/j.revmed.2013.02.030. PMID 23523078.